Committee for Health, Social Services and Public Safety - 2007-2011 Mandate
Report on the Autism Bill
Report on the Autism Bill.pdf (3.77 mb)
Health, Social Services and Public Safety Committee
Report on the Autism Bill
Together with the Minutes of Proceedings, Minutes of Evidence and
Written Submissions Relating to the Report
Ordered by The Health, Social Services and Public Safety Committee to be printed 10 February 2011
Report: NIA 43/10/11R Health, Social Services and Public Safety Committee
Session 2010/2011
Third Report
Membership and Powers
The Committee for Health, Social Services and Public Safety is a Statutory Departmental Committee established in accordance with paragraphs 8 and 9 of the Belfast Agreement, section 29 of the Northern Ireland Act 1998 and under Standing Order 48.
The Committee has power to:
- Consider and advise on Departmental budgets and annual plans in the context of the overall budget allocation;
- Consider relevant secondary legislation and take the Committee stage of primary legislation;
- Call for persons and papers;
- Initiate inquiries and make reports; and
- Consider and advise on any matters brought to the Committee by the Minister for Health, Social Services and Public Safety
The Committee has 11 members including a Chairperson and Deputy Chairperson and a quorum of 5.
The membership of the Committee is as follows:
Mr Jim Wells (Chairperson)
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Mickey Brady
Mr Pól Callaghan
Dr Kieran Deeny
Mr Alex Easton
Mr Tommy Gallagher
Mr Sam Gardiner
Mr Paul Girvan
Mr John McCallister
Ms Sue Ramsey
[1]With effect from 20 May 2008 Mrs Claire McGill replaced Ms Carál Ní Chuilín.
With effect from 15 September 2008 Mr Sam Gardiner replaced Rev Dr Robert Coulter.
With effect from 29 June 2009 Mrs Dolores Kelly replaced Mr Tommy Gallagher
With effect from 4 July 2009 Mr Jim Wells replaced Mrs Iris Robinson
With effect from 14 September 2009 Mrs Iris Robinson replaced Mr Thomas Buchanan
With effect from 12 January 2010 Mrs Iris Robinson resigned as an MLA
With effect from 15 January 2010 Mrs Carmel Hanna resigned as an MLA
With effect from 26 January 2010 Mr Conall McDevitt replaced Mrs Carmel Hanna
With effect from 1 February 2010 Mr Thomas Buchanan replaced Mrs Iris Robinson
With effect from Monday 24 May 2010 Mr Tommy Gallagher replaced Mr Conall McDevitt
With effect from Monday 24 May 2010 Mrs Mary Bradley replaced Mrs Dolores Kelly
With effect from Monday 13 September 2010 Mr Mickey Brady replaced Mrs Claire McGill
With effect from Monday 13 September 2010 Mr Paul Girvan replaced Mr Thomas Buchanan
With effect from Monday 23 November 2010 Mr Pól Callaghan replaced Mrs Mary Bradley
Table of Contents
Clause by Clause consideration of the Bill
Appendix 1:
Appendix 2:
Appendix 3:
Appendix 4:
Appendix 5:
Appendix 6:
Executive Summary
The purpose of the Bill is to enhance the provision of services to and support for people with conditions which are on the autistic spectrum. It does so by amending the Disability Discrimination Act 1995 (DDA) so as to resolve any ambiguity as to whether the term "disability" applies to autistic spectrum disorder (ASD), and by requiring the preparation of a cross-departmental autism strategy.
The evidence from the stakeholders was wide-ranging and many different views on the Bill were expressed. Some organisations welcomed the Bill in its entirety, others had concerns with particular clauses, while some groups opposed the Bill completely.
The first key issue for the Committee was in relation to clause 1 of the Bill. Clause 1 seeks to amend both the definition of disability as set out in the DDA and the list of "normal day to day activities" contained in Schedule 1 of the DDA. In overall terms, some organizations supported this clause because they took the view that it would enhance the ability of those people with ASD to claim protection under the DDA. However, other groups held the opposite view and argued that any changes to the DDA could potentially exclude those same people from its protection.
The Committee suggested to the Sponsor of the Bill, Mr Bradley MLA, that to amend the current definition of disability as a "physical or mental impairment" could in fact narrow the scope of people who could fall within the definition of disability. Mr Bradley accepted the Committee's view and agreed to draft an amendment to leave out clause 1 (2) of the Bill.
In relation to clause 1 (3) of the Bill which seeks to expand on the list of "day to day activities" contained in the DDA, the Committee took the view that the Bill was following a similar approach to that contained in guidance currently being consulted upon for the Equality Act 2010. The Committee agreed it was content with this clause as drafted.
The second key issue concerned the preparation of an autism strategy. Some stakeholders argued that legislation is required to ensure that all government departments work in a joined up manner to produce a comprehensive strategy to deal with ASD. Other organisations took the view that the current departmental strategies were working well and that a new strategy would result in more bureaucracy. The Committee came to the view that a legislative requirement for all government departments to co-operate in the production of an autism strategy was a positive step forward and would ensure input from all departments.
The third key issue concerned the content of the autism strategy. Clause 3 (5) of the Bill requires autism awareness training for civil servants who deal directly with the public. Concerns were expressed by stakeholders that this would have significant cost implications. The Committee suggested that training might be better directed at frontline public sector workers in the fields of health and education rather than at civil servants. Mr Bradley accepted the Committee's view that the clause was problematic and agreed to draft an amendment to leave out clause 3 (5) of the Bill.
Introduction
The Autism Bill (NIA 2/10) was referred to the Committee in accordance with Standing Order 33 on completion of the Second Stage of the Bill on 7th December 2010.
The Sponsor of the Bill, Mr Dominic Bradley MLA made the following statement under Standing Order 30:
"In my view the Autism Bill would be within the legislative competence of the Northern Ireland Assembly."
The stated purpose of the Bill is to enhance the provision of services to and support for people with conditions which are on the autistic spectrum. The Bill will amend the Disability Discrimination Act 1995 and require an autism strategy to be prepared.
During the period covered by this report, the Committee considered the Bill and related issues at eight meetings. The relevant extracts from the Minutes of Proceedings for these meetings are included at Appendix 1.
The Committee had before it the Autism Bill (NIA 2/10) and the Explanatory and Financial Memorandum that accompanied the Bill.
The Committee agreed a motion to extend the Committee Stage of the Bill to 11 February 2011. The motion to extend was supported by the Assembly on 24 January 2011.
On referral of the Bill the Committee wrote on 10 December 2010 to key stakeholders and inserted public notices in the Belfast Telegraph, Irish News and News Letter seeking written evidence on the Bill by 6 January 2011.
A total of 33 organisations responded to the request for written evidence and copies of the submissions received by the Committee are included at Appendix 3.
The Committee took oral evidence from:
- The Regional Autism Spectrum Disorder Network and Autism NI/ Parents Autism Lobby on 16 December 2010.
- Autism Initiatives, the National Autistic Society and the Parents' Education as Autism Therapists (PEAT) on 13 January 2011.
- The Department of Education, the Department for Health, Social Services & Public Safety, the Regional Autism Spectrum Disorder Network Reference Group and the Bill's Sponsor Mr Dominic Bradley MLA on 20 January 2011.
The Minutes of Evidence of these sessions are included at Appendix 2.
The Committee carried out clause by clause scrutiny of the Bill on 27 January 2011.
At its meeting on 10 February 2011 the Committee agreed its report on the Bill and that it should be printed.
Consideration of the Bill by the Committee
Background
Autism Spectrum Disorder (ASD) is a complex developmental condition that essentially affects the way a person communicates and relates to people.
People with autism generally experience three main areas of difficulty, which are commonly referred to as 'the triad of impairments'.
- Social interaction (difficulty with relationships, for example appearing aloof and indifferent to other people).
- Social communication (difficulty with verbal and non-verbal communication, for example not fully understanding the meaning of common gestures, facial expressions or tone of voice).
- Imagination (difficulty in the development of interpersonal play and imagination, for example having a limited range of imaginative activities, possibly copied and pursued repetitively).
The Autism Bill was proposed by Mr Dominic Bradley MLA, chairperson of the All-Party Assembly Group on Autism which was formed in 2008 to attempt to inform Assembly Members about autism issues.
Proposals for the Bill were developed as a consequence of the work of the group and its engagement with stakeholders.
The All-Party Assembly Group on Autism decided that it was important to advocate a cross-departmental regional strategy for ASD, linked to, and supported by, legislation.
The Bill has 7 clauses and no schedules.
Key Issues
Clause 1 - Amendment to the Disability Discrimination Act (DDA) 1995
The Bill's Sponsor Mr Dominic Bradley stated the aim of amending the DDA was to clarify that people with ASD fell within its scope. In his view, there is an ambiguity as to whether those people on the autistic spectrum are current covered by the DDA and this can have a detrimental effect on their ability to access services and benefits.
During an oral evidence session prior to the introduction of the Bill on 14 October 2010, Mr Bradley explained the purpose of clause 1 as follows:
'To ensure that ASD is included, it amends the definition of disability in the existing Disability Discrimination Act (DDA) 1995 by inserting: "social (including communication)". The draft Bill, therefore, provides more clarity for the Departments and public bodies that use the DDA definition of disability as guidance when making decisions, for example, on disability living allowance (Appendix 2)'.
A number of organisations supported Mr Bradley's stance on the need to amend the DDA including Autism NI, the Human Rights Commission, Autism Initiatives, Action for Children and the Parent's Autism Lobby (PAL).
However, other groups held the opposite view and argued against any changes to the DDA. These groups included the Department of Health, Social Services and Public Safety (DHSSPS), the Regional Autism Spectrum Disorder Network (RASDN), the Reference Group of RASDN, the Health and Social Care (HSC) Board, Aspergers Network, the Equality Commission, a number of the Education and Library Boards, Carers NI, the Royal College of Speech and Language Therapists, the Royal College of General Practitioners, and a number of the (Health and Social Care) HSC Trusts.
Many of these groups were of the opinion that ASD was already covered by the DDA and that amending the DDA would not have the desired effect of increasing access to social security benefits. During oral evidence on 20 January 2011 the DHSSPS stated:
'The Department believes that autism is covered by the current DDA, which is evidenced by case law, and I am happy to talk about case law if you want me to. The Office of the First Minister and deputy First Minister guidance on the existing DDA clearly states that autism is covered (Appendix 2)'.
Similarly, oral evidence from the Regional Autism Spectrum Disorder Network on 16 December 2010 supported this view:
'Our perception is that the Children Order and the DDA are all-encompassing. It is of concern to us that the focus would be on specific conditions rather than on the broad spectrum of people with a disability. We should look across our services — universal services as well as specialist services — to support people with disabilities who live in our communities.
We contest the notion that not including autism in the DDA creates inequalities (Appendix 2)'.
At its meeting on 20 January 2011 the Committee considered a research paper (Appendix 4) which indicated that the term 'physical or mental impairment' had intended to be all encompassing when the DDA was originally introduced. The paper also noted that a view had been put forward in other jurisdictions that to amend the term "physical or mental impairment" could in fact narrow the scope of people who could fall within the definition of disability.
When the Committee took evidence from Mr Bradley on the Bill, it raised the issues of concern relating to clause 1. Mr Bradley advised the Committee that he had further considered the issue of amending the definition of disability and had come to the decision leave out clause 1 (2) from the Bill. The Committee welcomed Mr Bradley's amendment to the Bill.
The need to legislate for an Autism Strategy
Mr Bradley stated that there is a lack of co-ordination currently between the Department of Education and Department of Health, Social Services and Public Safety in terms of delivering strategies to address the needs of people with ASD. In his view legislation is required to ensure that all government departments work in a joined up manner to produce a comprehensive strategy to deal with ASD.
This position was supported by Autism NI, the College of Occupational Therapists, Autism Initiatives, Action for Children, Carers NI and the Parent's Autism Lobby.
For example Autism NI stated during oral evidence on 16 December 2010:
'We believe that the legislation can only strengthen and empower that which is already happening. At the moment, there is limited buy-in from other Departments. The DHSSPS ASD strategy relies on a medical model, not a social model. The balance of resources has gone into diagnosis and not into early intervention or family support (Appendix 2)'.
Likewise, Autism Initiatives indicated during oral evidence on 13 January 2011 that it supported an autism strategy across the full range of Government departments and activities:
'There is a level of co-operation, but, particularly at a time of acute financial difficulty, it is much easier for other Departments to prioritise other areas or reduce services in some areas. A legislative commitment would make it more difficult for that to happen. That is one of the main reasons why we support that approach (Appendix 2).'
However, other groups expressed concerns about the legislative requirement for an autism strategy including the DHSSPS, RASDN, the HSC Board, the Human Rights Commission, The Parent Carers' Council on Disability, a number of the Education and Library Boards, the Equality Commission, and a number of the HSC Trusts.
For example, during oral evidence on 16 December 2010 the Regional Autism Spectrum Disorder Network indicated that co-operation between agencies already existed without the need for legislation:
'The board believes that integrated planning across agencies and Departments is critical to meeting the wide-ranging need of anyone with a disability, including people with autism, as a principle. An example of that is through children's services planning, which is a mechanism that we employ. Currently, there is no statutory duty to co-operate under children's services planning, but we have an effective, multi-agency planning system that has been running for nearly 12 years (Appendix 2)'.
The Regional Autism Spectrum Disorder Network Reference Group supported this view and in its written submission stated:
'The Department has already carried out an Independent Review of Autism Services and is a year into implementing the Review's recommendations. It is, literally, involving parents, carers and users at Trust level in all aspects of service provision including 'commissioning'' (Appendix 3).
After considering the evidence the Committee came to the view that a legislative requirement for all government departments to co-operate in the production of an autism strategy was a positive step forward. It was the Committee's view that without legislation it would be difficult to ensure that departments other than health and education fully participated in the strategy.
Cost of an Autism Strategy
In terms of the content of the autism strategy, a number of stakeholders raised concerns in relation to the potential financial implications.
The DHSSPS had specific concerns regarding the costs associated with clause 3 (5) which deals with the provision of autism awareness training for civil servants who deal directly with the public. The Department indicated in its written submission:
'Training for civil servants brings a potential cost of some £1.8m (based on circa 25,500 civil servants at £65 per head)' (Appendix 3).
Likewise, the Minister for Finance & Personnel raised the matter of cost in his written submission which stated:
' I share Mr McGimpsey's concerns particularly about the lack of information on costs and the absence of a finance clause taking account of direct and wider impacts on funding (Appendix 3)'.
Similarly, the Aspergers Network in its written evidence stated:
'No financial effects are available, and considering the Bill requires public servants, who deal with the public are to be trained; at what cost. Will these costs be removed from the recent increase in Trust services for families? Or would there be a decrease in the new Autism related jobs within Trusts? (Appendix 3)'.
However, other groups such as Autism NI made the counter argument and suggested that a cohesive autism strategy may reduce costs:
'With an effective cross-departmental strategy, with good strong leadership at the head, the potential for cost saving through reduction of duplication is incredible (Appendix 2)'.
During his oral evidence on 20 January 2011, Mr Bradley disputed the Department's estimate of the cost of training civil servants:
'I presume that some of that cost is already being met by the system, because public servants in the Department of Education and the Department of Health, Social Services and Public Safety already receive some autism training. A level of training is probably provided by other Departments, such as the Department for Social Development, although that may not be sufficient. That might be the global figure for the overall costs, but, as I said, some of that is already being incurred by Departments. There may be an extra cost, but it would not be at the level of £1·8 million (Appendix 2)'.
Mr Bradley further indicated during his evidence on 20 January 2011 that he was considering an amendment to change the reference from "civil servants" to "public servants". In response, the Minister for Health, Social Services & Public Safety wrote to the Committee in a letter dated 27 January 2011 to express the following concerns:
'My Department does not hold figures for public servants for the whole of NI; however for health and social care, there are approximately 71,300 public servants (at 31 December 2010). This proposed amendment would, therefore, increase this potential cost to circa £4.6m for this Department alone; this takes cognizance of the fact that some staff have already been trained in autism awareness. This does not include, PSNI, Council workers, teachers, bus drivers etc. who would be included in the figures from other Departments' (Appendix 4).
When Mr Bradley was made aware of these concerns he subsequently wrote to the Committee to advise that he intends to withdraw clause 3 (5) from the Bill completely (Appendix 4). The Committee was content with this amendment.
Summary of Evidence
General Comments
In considering the Bill, the Committee took account of the written and oral evidence received from the range of stakeholders who responded to its call for evidence. It also took oral evidence from the Sponsor of the Bill, Mr Dominic Bradley MLA, who provided additional information and clarification on the points raised in the submissions received.
The evidence received and considered by the Committee was wide-ranging and the views of organisations differed considerably towards the Bill. Many organisations welcomed the Bill in its entirety, however others had concerns with particular clauses, while some groups opposed the Bill completely.
Clause 1: Amendment to the Disability Discrimination Act (DDA) 1995
A broad spectrum of evidence was received on clause 1 of the Bill which seeks to amend both the definition of disability as set out in the DDA and the list of "normal day to day activities" contained in Schedule 1 of the DDA. In overall terms, some organisations supported this clause because they took the view that it would enhance the ability of those people with ASD to claim protection under the DDA. However, other groups held the opposite view and argued that any changes to the DDA could potentially exclude those same people from its protection.
The groups which supported clause 1 included Autism NI, the Human Rights Commission, Autism Initiatives, Action for Children and the Parent's Autism Lobby (PAL). Their view was that the addition of the words "social (including communication)" to the existing definition of disability as a "physical or mental impairment" would allow more people with ASD to be recognized as having a disability, and that this would enhance their access to services and benefits. Likewise, they believed that the extension of the list of "normal day to day activities" would help resolve any ambiguity as to whether the DDA covers people with ASD.
These stakeholders explained to the Committee that in their experience some government agencies relied on the DDA when assessing whether a person with ASD was entitled to various benefits, including Disability Living Allowance (DLA). The feeling was that the DDA in its present form does not provide sufficient clarity to decision makers on whether ASD falls within it.
The Northern Ireland Human Rights Commission came at the issue from a slightly different position. They supported the amendment to the definition of disability to include social and communication impairments. It was their view that given that the state has endorsed the Convention on the Rights of Persons with Disability's use of the social model of disability, the statutory definition should also reflect this position.
However, other organisations expressed serious concerns about the changes proposed to the DDA in the Bill. These included the DHSSPS, RASDN, the Reference Group of RASDN, the HSC Board, Aspergers Network, the Equality Commission, a number of the Education and Library Boards, Carers NI, the Royal College of Speech and Language Therapists, the Royal College of General Practitioners, and a number of the HSC Trusts.
The DHSSPS, RASDN and the HSC Board contended that the definition of disability within the DDA already covered people with ASD, and that the term "physical or mental impairment" was intended to be all-encompassing. The Aspergers Network took a similar stance and argued that to alter the definition of disability under the DDA may undermine the legal status of the DDA completely. Likewise, the Equality Commission advised that it was not aware that the definition of disability in the DDA had caused particular difficulties for people with autism accessing their rights under the legislation.
The DHSSPS also argued that amending the DDA as proposed by the Bill would not have the effect of increasing access to benefits such as DLA for those people with ASD. A research paper prepared for the Committee provided further information on this issue and made the point that the DDA only provides protection to those people who meet its definition of disability. This definition of disability is not applied within the benefits and tax credits systems (Appendix 4).
In terms of the education sector, a number of groups were concerned that clause 1 could give rise to possible conflicts with Special Educational Needs (SEN) legislation. The Department of Education advised the Committee that it was currently examining the potential impact of the Autism Bill on the current SEN legislation in terms of whether the Bill might give priority to children with autism over children with other SEN. However, they did not reach a conclusion on this matter before the completion of committee stage (Appendix 4).
The Royal College of Speech and Language Therapists objected to clause 1 on the basis that it may further discriminate against individuals with a communication disability who do not have a social communication disability.
Towards the end of its period of evidence taking, the Committee considered a research paper which noted that a view had been put forward in other jurisdictions that to amend the term "physical or mental impairment" could in fact narrow the scope of people who could fall within the definition of disability (Appendix 4).
In terms of the proposed amendment to the list of "day to day activities", the research paper advised that a consultation document had been published on guidance for defining disability within the context of the Equality Act 2010 (Appendix 4). The consultation paper included the following day to day activity – "Significant difficulty taking part in normal social interaction or forming social relationships". The Committee noted that this wording was very similar to what was being proposed in clause 1 (3) of the Bill.
When the Committee took evidence from Mr Bradley on the Bill, it raised the issues of concern relating to clause 1. Mr Bradley advised the Committee that he had further considered the issue of amending the definition of disability and had come to the decision leave out clause 1 (2) from the Bill. Mr Bradley then confirmed his position in writing to the Committee (Appendix 4). The Committee welcomed Mr Bradley's amendment to the Bill.
In terms of clause 1 (3) which amends the list of "day to day activities" in Schedule 1 of the DDA, the Committee noted that a similar approach was being taken in relation to the guidance being developed for the Equality Act 2010. The Committee was therefore content with clause 1 (3) of the Bill.
Clause 2: Autism Strategy
As with clause 1, opinion was divided amongst stakeholders on the merits or otherwise of legislating for an autism strategy.
Those who supported this clause made the general argument that legislation is required to ensure that all government departments work in a joined up manner to produce a comprehensive strategy to deal with ASD.
However, other organisations took the view that the current autism strategies being delivered by the DHSSPS and the Department of Education were working well, and that to create a new strategy would result in more bureaucracy. Furthermore, they argued that designing a new autism strategy would be costly in terms of time and money, and that resources would be better spent to provide services for people with ASD.
The groups which supported clause 2 included Autism NI, the College of Occupational Therapists, Autism Initiatives, Action for Children, Carers NI and the Parent's Autism Lobby.
Autism NI made the point that in relation to the current strategies being delivered by the DHSSPS and the Department of Education, there is limited buy-in from other departments. Autism Initiatives stated that making it a legislative requirement for departments to produce a joined up strategy on autism would be valuable, particularly at a time of public spending cut-backs. PAL stated that currently there was a lack of co-ordination between departments in relation to ASD which has resulted in both duplication and gaps in some services.
However, other groups expressed concerns about clause 2 including the DHSSPS, RASDN, the HSC Board, the Human Rights Commission, The Parent Carers' Council on Disability, a number of the Education and Library Boards, the Equality Commission, and a number of the Trusts.
The Equality Commission stated that while it is in favour of a cross departmental action plan, with actions, timescales and performance indicators, it is not convinced that there is clear need for the DHSSPS to be placed under a statutory duty to prepare a strategy on autism. Likewise, the BELB and NEELB support the need for interdepartmental and multi-agency co-operation in order to achieve a co-ordinated autism strategy, but were concerned that ASD specific legislation in relation to children could advertently discriminate against all other children with special needs. They suggested that the Bill be restricted to adult services only as has been done with the Autism Act 2009 in England.
The DHSSPS argued that from a policy perspective, it remains uncertain what the proposed strategy is designed to do, especially since there is already in place an ASD strategic action plan and an infrastructure to deliver it. This stance was also taken by the HSC Trusts. The Department also pointed to the issue of cost, and stated that it might be argued that the Bill's intent is to improve rights of individuals and their carers to have needs met and that this could not be achieved without significant cost.
RASDN made reference to the work it was already carrying out in terms of its ASD strategy and stated that they already work on a multi-agency basis. In their view this is recognised good practice and legislation is not required to force them to do it. The Reference Group of RASDN stated that the current strategy is working and progress is being made.
After considering the evidence the Committee came to the view that a legislative requirement for all government departments to co-operate in the production of an autism strategy was a positive step forward. It was the Committee's view that without legislation it would be difficult to ensure that departments other than Health and Education fully participated in the strategy.
The Committee agreed that it was content with clause 2.
Clause 3: Content of the Autism Strategy
As with the previous two clauses, opinions were divided on clause 3.
A number of organisations including Autism NI, Action for Children, the Parent's Autism Lobby, and the National Autistic Society supported clause 3. They argued that it was important that the strategy addresses the needs of people with ASD throughout their lives from childhood through to adulthood. They drew attention in particular to the key transition issues facing people with ASD, when they make the move from childhood towards adulthood and independence.
However, other organisations highlighted concerns regarding clause 3 such as the DHSSPS, the College of Occupational Therapists, Education and Library Boards and Autism Initiatives.
The DHSSPS stated in their evidence to the Committee that some concern has been expressed that the Autism Bill might possibly be subject to challenge under the European Convention on Human Rights, particularly in relation to individuals and families living with other significant disabling conditions. However, the Department did not provide any further information on what basis it was postulating this view.
A number of groups, including the Education and Library Boards, took the view that an autism strategy should only apply to adults. They suggested that if the autism strategy relates to children and young people it may give rise to complexities and possible conflicts with existing SEN legislation.
The Committee raised an issue with Mr Bradley in relation to clause 3 (2) in terms of the use of the word "social". The Committee questioned whether the term "social" needed to be expanded upon, to ensure that issues such as the employment or housing needs of people with ASD were covered in the strategy.
Mr Bradley wrote to the Committee to advise that he had taken advice on the interpretation of clause 3 (2) specifically relating to the possible advantage of elaborating on the meaning of the term "social" to include "employment, leisure, housing, etc". His advice was that clause 3 (2) must be read in light of the general overarching obligation in 3 (1). Clause 3 (2) therefore begins "Without prejudice to the generality of subsection 1" to clarify that these issues highlighted are not to diminish the wider obligation. In his view no specific amendment is required as the overall interpretation of clause 3 (2) is inclusive (Appendix 4).
The DHSSPS also raised the issue of cost and queried the fact that Mr Bradley had stated that the Bill would have no significant costs. The Department pointed to the fact that the cost of formulating a rolling and indefinite autism strategy is not specified, nor is the need to establish extensive monitoring arrangements. The Department of Finance and Personnel also expressed a concern about the lack of information on costs and the absence of a finance clause in the Bill taking account of direct and wider impacts on funding.
However, other groups such as Autism NI made the counter argument and suggested that a cohesive autism strategy would not only stop wasteful duplication of some services, but through appropriate interventions and support greatly reduce future costs on society as individuals and families are empowered to support themselves.
The DHSSPS had specific concerns regarding the costs associated with clause 3 (4) which requires it to set out proposals for promoting an autism awareness campaign, and clause 3 (5) which deals with the provision of autism awareness training for civil servants who deal directly with the public.
The Department advised that it had developed its own indicative costs. In relation to training for civil servants, the Department quoted a potential cost of some £1.8m (based on circa 25,500 civil servants at £65 per head). In relation to the potential cost of public awareness-raising, the Department quoted figures ranging from £25,000 for a small advertising campaign to £235,000 for a wider campaign encompassing limited TV, press, online and radio adverts.
Autism Initiatives also had concerns with costs, and stated that they would prefer to see the resources directed at a public awareness campaign and training for civil servants go to frontline services. In their view awareness raising and training could be carried out as part of general disability awareness campaigns.
The Committee was concerned with clause 3 (5) in terms of its reference to "civil servants". The view was that there were other public sector workers who delivered frontline services in health and social care and education who would benefit more from autism awareness training than civil servants would.
Mr Bradley subsequently wrote to the Committee to advise that he intends to withdraw clause 3 (5) from the Bill completely (Appendix 4). The Committee was content with this amendment.
Clause 4: Interpretation
The Committee received few comments in relation to this clause.
The Education and Library Boards stated that as the terminology surrounding autism changes and will continue to change over time, the Autism Bill should adopt a similar approach to the Autism Act 2009 by not including the definition of autism in the primary legislation.
The Committee agreed it was content with the clause.
Clause 5: Regulations and Orders made under this Act
The Committee did not receive any comments in relation to this clause.
Clause 6: Commencement
The Committee did not receive any comments in relation to this clause.
Clause 7: Short Title
The Committee did not receive any comments in relation to this clause.
Clause by Clause Consideration of the Bill
The Committee undertook its clause by clause scrutiny of the Bill on 27 January 2011 – see Minutes of Evidence in Appendix 2.
Clause 1: Amendment to the Disability Discrimination Act 1995
The Committee indicated it was content with the clause as drafted subject to the proposed amendment agreed with the Sponsor of the Bill to withdraw clause 1 (2) which amends the definition of disability in the 1995 Act.
Clause 2: Autism strategy
The Committee indicated it was content with the clause as drafted.
Clause 3: Content of the Autism Strategy
The Committee indicated it was content with the clause as drafted subject to the proposed amendment agreed with the Sponsor of the Bill to withdraw clause 3 (5) which deals with autism awareness training for Northern Ireland Civil Service Staff who deal directly with the public.
Clause 4: Interpretation
The Committee indicated it was content with the clause as drafted.
Clause 5: Regulations and Orders made under this Act
The Committee indicated it was content with the clause as drafted.
Clause 6: Commencement
The Committee indicated it was content with the clause as drafted.
Clause 7: Short Title
The Committee indicated it was content with the clause as drafted.
Long Title
The Committee indicated it was content with the long title of the Bill as drafted.
Appendix 1
Minutes of Proceedings
Thursday, 14 October 2010
Room 30, Parliament Buildings
Present: Mr Jim Wells MLA (Chairperson)
Mrs Mary Bradley MLA
Mr Mickey Brady MLA
Dr Kieran Deeny MLA
Mr Alex Easton MLA
Mr Tommy Gallagher MLA
Mr Sam Gardiner MLA
Mr John McCallister MLA
Mrs Michelle O'Neill MLA (Deputy Chairperson)
Ms Sue Ramsey MLA
In Attendance: Dr Kathryn Bell (Clerk)
Mr Mark McQuade (Assistant Clerk)
Ms Leanne Johnston (Clerical Supervisor)
Mr Neil Sedgewick (Clerical Supervisor)
Mr Craig Mealey (Clerical Officer)
2.01 p.m The meeting commenced in public session.
1. Evidence session on Private Members Bill on Autism
The Committee took evidence from:
Mr Dominic Bradley MLA
Arlene Cassidy, Secretariat to All Party Assembly Group on Autism
A question and answer session ensued. The Chairperson thanked the witnesses for attending.
[EXTRACT]
Thursday, 2 December 2010
Room 30, Parliament Buildings
Present: Mr Jim Wells MLA (Chairperson)
Mr Pól Callaghan MLA
Mr Alex Easton MLA
Mr Tommy Gallagher MLA
Mr Sam Gardiner MLA
Mr Paul Girvan MLA
Mr John McCallister MLA
Ms Sue Ramsey MLA
Apologies: Dr Kieran Deeny MLA
Mrs Michelle O'Neill MLA (Deputy Chairperson)
In Attendance: Dr Kathryn Bell (Clerk)
Mr Mark McQuade (Assistant Clerk)
Ms Leanne Johnston (Clerical Supervisor)
Mr Craig Mealey (Clerical Officer)
2.00 p.m The meeting commenced at in public session.
1. Evidence session on Autism Bill with departmental officials
The Committee took evidence from
Dr Maura Briscoe Mental Health & Disability Policy Directorate, DHSSPS
Dr Ian McMaster Medical Officer, DHSSPS
Dr Hilary Harrison Social Services Officer, DHSSPS
Mr Peter Deazley Learning Disability Unit, DHSSPS
[EXTRACT]
Thursday, 9 December 2010
Room 30, Parliament Buildings
Present: Mr Jim Wells MLA (Chairperson)
Mr Mickey Brady MLA
Mr Alex Easton MLA
Mr Tommy Gallagher MLA
Mr Sam Gardiner MLA
Mr John McCallister MLA
Mrs Michelle O'Neill MLA (Deputy Chairperson)
Ms Sue Ramsey MLA
Apologies: Mr Pól Callaghan MLA
Dr Kieran Deeny MLA
Mr Paul Girvan MLA
In Attendance: Dr Kathryn Bell (Clerk)
Mr Mark McQuade (Assistant Clerk)
Ms Leanne Johnston (Clerical Supervisor)
Mr Craig Mealey (Clerical Officer)
Mr Colin Pigeon (Assembly Research)
2.14 p.m. The meeting commenced in public session.
5. Autism Bill NIA 2/10
The Committee discussed the committee stage of the Autism Bill and agreed a motion to extend this until Friday 11th February 2011.
The Committee also agreed witnesses to be invited to present oral evidence to the Committee, organisations invited to submit written evidence to the committee and a public notice calling for evidence on the Bill.
The Committee agreed to meet on the mornings of 13 & 20 January to take oral evidence on the Bill.
The Committee agreed to write to the Department to seek information regarding the advice it is seeking from the Attorney General on the Bill.
[EXTRACT]
Thursday, 16 December 2010
Room 30, Parliament Buildings
Present: Mr Jim Wells MLA (Chairperson)
Mr Mickey Brady MLA
Mr Pól Callaghan MLA
Dr Kieran Deeny MLA
Mr Alex Easton MLA
Mr Tommy Gallagher MLA
Mr Paul Girvan MLA
Mr John McCallister MLA
Mrs Michelle O'Neill MLA (Deputy Chairperson)
Ms Sue Ramsey MLA
Apologies: Mr Sam Gardiner MLA
In Attendance: Dr Kathryn Bell (Clerk)
Mr Mark McQuade (Assistant Clerk)
Ms Leanne Johnston (Clerical Supervisor)
Mr Neil Sedgewick
Mr Craig Mealey (Clerical Officer)
Mr Tim Moore (Assembly Research)
Dr Janice Thompson (Assembly Research)
2.06 p.m The meeting commenced at in public session.
1. Autism Bill NIA 2/10
The Committee received a briefing from Assembly Research on the Autism Bill.
Evidence session with the Regional Autism Spectrum Disorder Network
The Committee took evidence from:
Mrs Fionnuala Mc Andrew Director of Social Care & Children, Health & Social Care Board
Dr Stephen Bergin Chair, Regional Autism Spectrum Disorder Network, Public Health Agency
Mr Kieran McShane Commissioning Head, Children and Families, Health & Social Care Board & Regional Autism Spectrum Disorder Network project team member
A question and answer session ensued. The Chairperson thanked the witnesses for attending.
5. Evidence session with Autism NI/ Parents Autism Lobby
The Committee took evidence from:
Ms Arlene Cassidy Chief Executive, Autism NI
Ms Paula Hanratty Director of Family Support, Autism NI
Ms Audrey Mullan Autism Resource Officer, Autism NI
Mr David Heatley Chairperson, Parents Autism Lobby
A question and answer session ensued. The Chairperson thanked the witnesses for attending.
[EXTRACT]
Thursday, 13 January 2011
Senate Chamber, Parliament Buildings
Present: Mr Jim Wells MLA (Chairperson)
Mr Mickey Brady MLA
Mr Pól Callaghan MLA
Mr Alex Easton MLA
Mr Tommy Gallagher MLA
Mr Paul Girvan MLA
Mr John McCallister MLA
Mrs Michelle O'Neill MLA (Deputy Chairperson)
Ms Sue Ramsey MLA
Mr Sam Gardiner MLA
Apologies: Dr Kieran Deeny MLA
In Attendance: Dr Kathryn Bell (Clerk)
Mr Mark McQuade (Assistant Clerk)
Ms Leanne Johnston (Clerical Supervisor)
Mr Neil Sedgewick (Clerical Supervisor)
Mr Craig Mealey (Clerical Officer)
Dr Lesley- Ann Black (Assembly Research)
1. Autism Bill NIA 2/10
The Committee agreed to ask Research Services to prepare a paper on clause 1 of the Bill based on the issues raised in the written submissions.
The Committee agreed to invite the Reference Group for the Regional Autistic Spectrum Disorder Network to give oral evidence at its next meeting.
The Committee noted correspondence from the Aspergers Network and agreed not to invite the group to provide oral evidence due to time constraints.
The Committee noted a document 'The Cost of Autism' from Autism NI.
The Committee noted correspondence from the Examiner of Statutory Rules regarding the delegated powers in the Autism Bill and agreed to forward this to Dominic Bradley MLA for his consideration.
2. Autism Bill NIA 2/10: Evidence session with Autism Initiatives
The Committee took evidence from:
Mr Alan Hanna Assistant Director, Autism Initiatives
Ms Grainne Close Assistant Director, Autism Initiatives
A question and answer session ensued. The Chairperson thanked the witnesses for attending.
3. Autism Bill NIA 2/10: Evidence session with the National Autistic Society
The Committee took evidence from:
Ms Regina Cox Co-Director National Autistic Society NI
Ms Shirelle Stewart Co-Director National Autistic Society NI
A question and answer session ensued. The Chairperson thanked the witnesses for attending
4. Autism Bill NIA 2/10 – Evidence session with Parents' Education as Autism Therapists (PEAT)
The Committee took evidence from:
Dr Tony Byrne Chairperson, Parents' Education as Autism Therapists (PEAT)
Ms Karen Gallagher Parents' Education as Autism Therapists (PEAT)
A question and answer session ensued. The Chairperson thanked the witnesses for attending.
[EXTRACT]
Thursday, 20 January 2011
Room 21, Parliament Buildings
Room 30, Parliament Buildings
Present: Mr Jim Wells MLA (Chairperson)
Mr Mickey Brady MLA
Mr Pól Callaghan MLA
Dr Kieran Deeny MLA
Mr Alex Easton MLA
Mr Tommy Gallagher MLA
Mr Paul Girvan MLA
Mr John McCallister MLA
Mrs Michelle O'Neill MLA (Deputy Chairperson)
Ms Sue Ramsey MLA
Mr Sam Gardiner MLA
In Attendance: Dr Kathryn Bell (Clerk)
Mr Mark McQuade (Assistant Clerk)
Ms Leanne Johnston (Clerical Supervisor)
Mr Neil Sedgewick (Clerical Supervisor)
Mr Craig Mealey (Clerical Officer)
Mr Tim Moore (Assembly Research)
Mr Colin Pidgeon (Assembly Research)
11.15 a.m. The meeting commenced in public session.
1. Autism Bill NIA 2/10
The Committee noted that a motion to extend the committee stage of the Bill would be considered by the Assembly on Monday 24th January 2011.
The Committee noted a response from the Minister regarding legal advice on the Bill.
The Committee agreed to publish written submissions received on the Bill on the Committee website.
2. Autism Bill NIA 2/10: Evidence session with the Department of Education
The Committee took evidence from:
Ms Dorothy Angus Director of Access, Inclusion and Well-Being, Department of Education
Ms Debbie Gladwell Head of Special Education Policy Advisory Team, Department of Education
Ms Gillian Boyd Department of Education
A question and answer session ensued. The witnesses agreed to provide the Committee with additional information. The Chairperson thanked the witnesses for attending.
3. Autism Bill NIA 2/10: Evidence session with the Department for Health, Social Services & Public Safety
The Committee took evidence from:
Dr Maura Briscoe Director of Mental Health & Disability Policy Directorate
Mr Peter Deazley Mental Health & Disability Policy Directorate
Mr Charles Bamford Social Services Officer
Dr Ian McMaster Medical Officer
A question and answer session ensued. The Chairperson thanked the witnesses for attending.
The Committee agreed to seek legal advice on the Autism Bill.
4. Autism Bill NIA 2/10: Briefing from Assembly Research
The Committee received a briefing from Tim Moore of Assembly Research on the Autism Bill.
5. Autism Bill NIA 2/10: Evidence session with RASDN Reference Group
The Committee took evidence from:
The Lord Maginnis of Drumglass Chairperson, RASDN Reference Group
Ms Laura Collins Parent/ Carer representative, RASDN Reference Group
Ms Nuala White Parent/ Carer representative, RASDN Reference Group
A question and answer session ensued. The Chairperson thanked the witnesses for attending
6. Autism Bill 2/10: Evidence session with Dominic Bradley MLA
The Committee took evidence from:
Mr Dominic Bradley MLA
Ms Arlene Cassidy Secretariat to All Party Assembly Group on Autism
A question and answer session ensued. The witnesses agreed to consider amendments to the Bill and provide details of these to the Committee for its next meeting. The Chairperson thanked the witnesses for attending.
[EXTRACT]
Thursday, 27 January 2011
Room 29, Parliament Buildings
Room 30, Parliament Buildings
Present: Mr Jim Wells MLA (Chairperson)
Mr Mickey Brady MLA
Mr Pól Callaghan MLA
Dr Kieran Deeny MLA
Mr Alex Easton MLA
Mr Tommy Gallagher MLA
Mr Paul Girvan MLA
Mr John McCallister MLA
Mrs Michelle O'Neill MLA (Deputy Chairperson)
Ms Sue Ramsey MLA
Mr Sam Gardiner MLA
In Attendance: Dr Kathryn Bell (Clerk)
Mr Mark McQuade (Assistant Clerk)
Ms Leanne Johnston (Clerical Supervisor)
Mr Neil Sedgewick (Clerical Supervisor)
Mr Craig Mealey (Clerical Officer)
Ms Alice McKelvey (Legal Advisor)
11.08 am The meeting commenced in closed session.
1. Autism Bill NIA 2/10: Consideration of legal advice
The Committee considered legal advice regarding the Autism Bill NIA 2/10.
11.20 a.m. Ms Sue Ramsey left the meeting.
11.29 a.m. Mr Alex Easton left the meeting.
11.35 a.m. Ms Sue Ramsey rejoined the meeting.
11.36 a.m. Mr Alex Easton rejoined the meeting.
11.54 a.m. Mr Paul Girvan left the meeting.
11.57 a.m. Mr Tommy Gallagher left the meeting.
11.57 a.m. Mr Pól Callaghan left the meeting.
11.59 a.m. The meeting moved to public session.
2. Autism Bill NIA 2/10: Informal clause by clause consideration
The Committee noted correspondence from Lord Maginnis.
The Committee noted two FOI requests.
The Committee noted correspondence from the Minister.
The Committee noted correspondence from Dominic Bradley MLA.
The Committee discussed the Autism Bill.
12.00 p.m. Mrs Michelle O'Neill left the meeting.
12.09 p.m. Mrs Michelle O'Neill rejoined the meeting.
12.09 p.m. Mr Tommy Gallagher rejoined the meeting.
12.09 p.m. Mr Pól Callaghan rejoined the meeting.
12.55 p.m. Meeting adjourned.
2.10 p.m. Meeting resumed.
3. Autism Bill NIA 2/10: clause by clause consideration
3.14 p.m. Ms Sue Ramsey left the meeting.
The Committee noted further correspondence from Mr Dominic Bradley MLA regarding the Bill.
Clause 1 - Amendment to the Disability Discrimination Act 1995
The Committee divided: Ayes 6; Noes 0; Abstentions 3
AYES
- Mr Mickey Brady
- Mr Pól Callaghan
- Mr Alex Easton
- Mr Tommy Gallagher
- Mr Paul Girvan
- Mrs Michelle O'Neill
ABSTENTIONS
- Mr Sam Gardiner
- Mr John McCallister
- Mr Jim Wells
Question: That the Committee is content with the clause subject to the proposed amendment agreed with the sponsor, put and agreed to.
Clause 2 - Autism strategy
The Committee divided: Ayes 6; Noes 0; Abstentions 3
AYES
- Mr Mickey Brady
- Mr Pól Callaghan
- Mr Alex Easton
- Mr Tommy Gallagher
- Mr Paul Girvan
- Mrs Michelle O'Neill
ABSTENTIONS
- Mr Sam Gardiner
- Mr John McCallister
- Mr Jim Wells
Question: That the Committee is content with the clause as drafted, put and agreed to.
3.20 p.m. Ms Sue Ramsey rejoined the meeting.
Clause 3 - Content of the autism strategy
The Committee divided: Ayes 7; Noes 0; Abstentions 3
AYES
- Mr Mickey Brady
- Mr Pól Callaghan
- Mr Alex Easton
- Mr Tommy Gallagher
- Mr Paul Girvan
- Mrs Michelle O'Neill
- Ms Sue Ramsey
ABSTENTIONS
- Mr Sam Gardiner
- Mr John McCallister
- Mr Jim Wells
Question: That the Committee is content with the clause subject to the proposed amendment agreed with the sponsor, put and agreed to.
Clause 4 - Interpretation
The Committee divided: Ayes 7; Noes 0; Abstentions 3
AYES
- Mr Mickey Brady
- Mr Pól Callaghan
- Mr Alex Easton
- Mr Tommy Gallagher
- Mr Paul Girvan
- Mrs Michelle O'Neill
- Ms Sue Ramsey
ABSTENTIONS
- Mr Sam Gardiner
- Mr John McCallister
- Mr Jim Wells
Question: That the Committee is content with the clause as drafted, put and agreed to.
Clause 5 - Regulations and orders made under this Act
The Committee divided: Ayes 7; Noes 0; Abstentions 3
AYES
- Mr Mickey Brady
- Mr Pól Callaghan
- Mr Alex Easton
- Mr Tommy Gallagher
- Mr Paul Girvan
- Mrs Michelle O'Neill
- Ms Sue Ramsey
ABSTENTIONS
- Mr Sam Gardiner
- Mr John McCallister
- Mr Jim Wells
Question: That the Committee is content with the clause as drafted, put and agreed to.
Clause 6 - Commencement
The Committee divided: Ayes 7; Noes 0; Abstentions 3
AYES
- Mr Mickey Brady
- Mr Pól Callaghan
- Mr Alex Easton
- Mr Tommy Gallagher
- Mr Paul Girvan
- Mrs Michelle O'Neill
- Ms Sue Ramsey
ABSTENTIONS
- Mr Sam Gardiner
- Mr John McCallister
- Mr Jim Wells
Question: That the Committee is content with the clause as drafted, put and agreed to.
3.25 p.m. Dr Kieran Deeny rejoined the meeting.
Clause 7 - Short title
The Committee divided: Ayes 7; Noes 0; Abstentions 4
AYES
- Mr Mickey Brady
- Mr Pól Callaghan
- Mr Alex Easton
- Mr Tommy Gallagher
- Mr Paul Girvan
- Mrs Michelle O'Neill
- Ms Sue Ramsey
ABSTENTIONS
- Dr Kieran Deeny
- Mr Sam Gardiner
- Mr John McCallister
- Mr Jim Wells
Question: That the Committee is content with the clause as drafted, put and agreed to.
Long Title
The Committee divided: Ayes 7; Noes 0; Abstentions 4
AYES
- Mr Mickey Brady
- Mr Pól Callaghan
- Mr Alex Easton
- Mr Tommy Gallagher
- Mr Paul Girvan
- Mrs Michelle O'Neill MLA
- Ms Sue Ramsey
ABSTENTIONS
- Dr Kieran Deeny
- Mr Sam Gardiner
- Mr John McCallister
- Mr Jim Wells
Question: That the Committee is content with the long title of the Bill, put and agreed to.
3.27 p.m. Mr Tommy Gallagher left the meeting.
3.28 p.m. Mr Pól Callaghan left the meeting.
[EXTRACT]
Thursday, 10 February 2011
Room 30, Parliament Buildings
Present: Mr Jim Wells MLA (Chairperson)
Mr Mickey Brady MLA
Mr Pól Callaghan MLA
Mr Alex Easton MLA
Mr Tommy Gallagher MLA
Mr Sam Gardiner MLA
Mr Paul Girvan MLA
Mr John McCallister MLA
Mrs Michelle O'Neill MLA (Deputy Chairperson)
Ms Sue Ramsey MLA
Apologies: Dr Kieran Deeny MLA
In Attendance: Dr Kathryn Bell (Clerk)
Mr Mark McQuade (Assistant Clerk)
Ms Leanne Johnston (Clerical Supervisor)
Mr Neil Sedgewick (Clerical Supervisor)
Mr Craig Mealey (Clerical Officer)
2.01 p.m. The meeting commenced in closed session.
2.19 p.m. The meeting moved to public session.
2.31 p.m. Mrs Michelle O'Neill rejoined the meeting.
2.41 p.m. Mr Jim Wells left the meeting.
2.41 p.m. Mrs Michelle O'Neill took the Chair.
1. Autism Bill NIA 2/10 – Consideration of Committee report
The Committee considered the Draft Report on the Committee Stage of the
Autism Bill paragraph by paragraph.
The Committee agreed the main body of the report:
Paragraphs 1 to 16, read and agreed.
Paragraphs 17 to 24, read and agreed.
Paragraphs 25 to 49, read and agreed.
Paragraphs 50 to 95, read and agreed.
Paragraphs 96 to 104, read and agreed.
The Committee agreed the Executive Summary:
Paragraphs 1-7, read and agreed.
The Committee agreed that the Committee Membership & Powers, table of contents and Appendices 1 to 6 be included in the report.
The Committee agreed that an extract of today's Minutes of Proceedings should be included in Appendix 1 of the report and were content that the Chairperson agrees the minutes relating to this.
The Committee agreed to order the Report on the Autism Bill NIA 2/10 to be printed.
2.43 p.m. Ms Sue Ramsey left the meeting.
2.45 p.m. Ms Sue Ramsey rejoined the meeting.
[EXTRACT]
Appendix 2
Minutes of Evidence
14 October 2010
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Mickey Brady
Dr Kieran Deeny
Mr Alex Easton
Mr Tommy Gallagher
Mr Sam Gardiner
Mr John McCallister
Ms Sue Ramsey
Witnesses:
|
Mr Dominic Bradley MLA |
All-Party Assembly Group on Autism Secretariat |
1. The Chairperson (Mr Wells): With us today are Dominic and Arlene, both of whom have been before the Committee on several occasions. Although Dominic Bradley needs little introduction to anyone in the room, he is an MLA for Newry and Armagh and chairperson of the all-party Assembly group on autism (APAGA). Arlene Cassidy is a member of the group's secretariat. As is usual, Dominic, you have 10 minutes in which to make an opening presentation, after which I will invite members to ask questions on the draft private Member's Bill.
2. Mr Dominic Bradley (All-Party Assembly Group on Autism Secretariat): Thank you for the opportunity to present evidence to the Committee on the draft autism Bill for Northern Ireland. We have been before the Committee on one previous occasion, and I am pleased to say that we have advanced the proposed Bill since then. The Committee has a copy of the draft Bill, and we intend to make few further changes to it. A single word or phrase here and there might change, but any further changes will be minimal.
3. I am the proposer of the draft Bill on behalf of the all-party group on autism. Arlene Cassidy is the chief executive of Autism NI and provides secretarial services to the group. Some members of the Committee, including Michelle O'Neill, are also members of the group. We sent a copy of our presentation to the Committee earlier, and it illustrates the tension between the unprecedented and rapid rise in the prevalence of autistic spectrum disorder (ASD) and the limited resources that are available to meet the resulting needs.
4. The case that I wish to put to the Committee today is that the historical failure to prioritise autism appropriately is compounded by the failure of existing legislation to recognise the disability. The draft Bill addresses that anomaly. To ensure that ASD is included, it amends the definition of disability in the existing Disability Discrimination Act (DDA) 1995 by inserting: "social (including communication)". The draft Bill, therefore, provides more clarity for the Departments and public bodies that use the DDA definition of disability as guidance when making decisions, for example, on disability living allowance.
5. The measure will profoundly affect families because it will accord recognition to a challenging condition that has been low in the hierarchy of disability in our society. When implemented across public bodies, it has the potential to improve the public understanding of issues that face individuals with ASD, such as access to services and buildings. Significantly, it will signal the beginning of the end of discrimination against individuals with ASD who have an IQ of above 70.
6. The draft Bill directs the establishment of a cross-departmental approach to ASD by requiring the development of a cross-departmental or government strategy for autism led by the Health Department. As I said, the historical failure to recognise ASD has resulted in a legacy of underfunding across Departments, and, as the amendment to the DDA takes effect, all Departments will, inevitably, have to address the impact of legislative change to their policies, practice and provision. Clause 2 creates the requirement to undertake that exercise together in an effort to minimise duplication and maximise effectiveness. I presume that there is consensus on the view that the development of a single departmental ASD strategy by the Health Department and, more recently, by the Education Department stands in sharp contrast to the joined-up realities of life as one transition leads to another across home, education, employment and community.
7. Given the climate of economic constraint, it is incumbent on all of us to plan smartly for future challenges. A cross-departmental commitment to joint planning for ASD is not only good practice, it also provides an opportunity to look afresh at existing resources and how they could be used or redeployed. It also challenges Departments to work innovatively with the voluntary sector to maximise the accountability, flexibility and creativity of all sectors.
8. The draft Bill addresses the issue of scrutiny. Just as there is an equality and financial balance to be struck between the entitlement to services and their cost, so there is a balance between the processes of accountability and bureaucracy. That clause recognises that challenge by placing a duty on the Minister of the designated lead Department to report to the Assembly every two years on the progress of the autism strategy.
9. The proposal to establish an autism advocate has been withdrawn, but it can be introduced in the future should the need arise. The withdrawal of the autism advocate from the Bill is a decision that we made in light of the present pressures on resources. The current accountability mechanisms, including this and other statutory Committees, along with the requirement of the Minister to report to the Assembly biennially will ensure accountability for the strategy. In light of the huge pressures on resources, the decision to withdraw the autism advocate is a responsible one.
10. After the all-party group's previous evidence session to the Committee on 17 September 2009, representatives from the Department of Health, Social Services and Public Safety raised concerns about the proposed legislation when they gave evidence on 1 October 2009. Their concerns focused on the perceived cost of the implementation of an autism Bill and on the impact that such legislation would have on other disability groups. It is our duty to listen to all views, as has been the policy of the all-party group since its inception in 2008, which was in response to the campaign led by families committed to change.
11. More recently, the consultation on the proposed legislation was conducted across a wide range of statutory and voluntary agencies and resulted in a positive rating of between 70% and 80%. Follow-up meetings were held with the Equality Commission, the Children's Commissioner and Disability Action. Those meetings resulted in agreed positions on the potential benefits attached to the introduction of the legislation in providing and enhancing clarity. In addition, the Northern Ireland Local Government Association (NILGA) and most of the 26 local councils passed unanimous motions in support of the draft Bill.
12. It is our position that the all-party group has, therefore, addressed the concerns expressed by the Department of Health, Social Services and Public safety and that the proposed autism Bill is deserving of support. We welcome the opportunity to present to you, and we would also welcome feedback from Committee members. I will finish there, and, once again, thank you for the opportunity to present our case.
13. The Chairperson: Thank you, Dominic, for your extremely helpful presentation. I would like clarification on a few points. Initially, there was a discussion about ring-fencing funding for those who have autism and those who care for them. That does not seem to feature in this draft. Was that an idea that was floated but did not come to anything? What is the position on funding?
14. Mr D Bradley: I will ask Arlene to respond to that.
15. Mrs Arlene Cassidy (All-Party Assembly Group on Autism Secretariat): Thank you. I remember the issue of ring-fenced funding as one of the three key messages of the political lobby that was led by Autism NI. In 2006, the three key aspirations of the political lobby were ring-fenced funding for autism, a cross-departmental strategy and an impact on legislation. Those were the aspirational goals of a political lobby; they were not signed up to per se by the all-party group.
16. The Chairperson: Does this draft Bill still leave it in the Minister's power to allocate funding for autism services as he deems appropriate?
17. Mr D Bradley: It will be the Minister's duty to co-ordinate the strategy across several Departments. Naturally, the Minister would not have power over any Department other than his own, but there would be a duty on him to provide the best possible services through the strategy and to meet the needs of those services with appropriate resources.
18. The Chairperson: Does any provision enable the Minister to do something that he cannot do currently should he so wish?
19. Mr D Bradley: Yes. At present, the Minister would probably find it difficult to formulate a cross-departmental strategy, as it would depend on the willingness of other Ministers to participate in and agree to it. From that perspective, the draft Bill gives the Minister added strength. It means that he does not have to depend on the goodwill of other Ministers, but that other Ministers are obliged to co-operate with him in formulating the strategy. From the point of view of the Health Minister, the draft Bill adds something to his armoury in relation to co-operation and linkages with other Departments.
20. Mr McCallister: Welcome, Dominic and Arlene. The Chairperson made a point about co-operation between Departments, and it will be no great surprise to the two of you, or to anyone around the table, to hear of my concerns about Middletown. How do you envisage the Minister linking into such a situation? It could almost be said that there is a divergence between the health and education policies on an autism strategy. This draft Bill does not give the Minister the power to intervene or to obtain resources from another Department. That concern is linked to some of the Chairperson's concerns about what the legislation will enable the Minister to do that he cannot do now. Even under the provisions of the draft Bill, he could not develop a strategy or demand resources if his plan was at odds with what the Minister of Education wanted to do.
21. Mr D Bradley: The Minister will outline what he believes to be an effective strategy, and the onus will be on other Departments to provide the resources to implement it.
22. Mrs Cassidy: If it is to be a cross-departmental strategy with a required sign-up by the other Ministers, all resources and plans would have to be reconciled. The other Ministers would be accountable to the Assembly should they not progress that strategy.
23. Mr McCallister: There could be potential difficulties with that because the structure of government means that all the Ministers might change next May. However, there the divergence in policy may remain, which could result in a worse position in which nothing happened. If the consensus that is required between Departments cannot be achieved, we could be left with a situation in which little or nothing happens, or, indeed, with a strategy that is weaker than what exists at present.
24. Mr D Bradley: That is probably the worst-case scenario. I do not choose to look at it that way. If that is an issue that needs to be addressed, we will certainly consider it. The Bill is still in draft form, and if there is a mechanism to overcome that scenario, we would welcome your views on it. All legislation must take account of the worst-case scenario and ensure that all possible loopholes are closed. I welcome the fact that you have apprised us of the issue.
25. The Chairperson: You have deleted the reference to an autism advocate, but left the door slightly ajar in the sense that it could be reconsidered. Would that require primary legislation, or does any provision in the draft Bill enable that to happen by way of a statutory rule or subordinate legislation?
26. Mr D Bradley: There is no such provision in this draft. You raised a good point; perhaps we need to consider including a reference to the autism advocate in the draft Bill. We did not do so because we considered that the accountability mechanisms in the Assembly should be strong enough to ensure the implementation of the strategy. Nevertheless, I note your point, which is useful, and we will consider it further.
27. Mrs O'Neill: I declare an interest as a member of the all-party group on autism. Another possibility is that there would be nothing to stop the Department, as part of the overarching strategy, proposing an advocate to oversee that strategy.
28. The Chairperson: However, for that person to be at the level of, for example, a commissioner would require primary legislation. We cannot simply decide that there will be an older people's commissioner or a children's commissioner; we have to go through all the required legal procedures. Bills were required to establish both of those posts.
29. Mr D Bradley: That is one reason why we have not included the advocacy role at this stage. The start-up costs would be considerable, and it would probably take a year or more to establish the office of advocate and its operation. As I said, we have not ruled out completely the role of advocate, and I take your point, Chairperson, that if consider it to be a future possibility, it may be judicious to include some opening in the draft Bill to facilitate it.
30. The Chairperson: That is a double-edged sword, because some people are keen on the idea of an advocate, and others are concerned about it. Its inclusion in the draft Bill as a potential option for the future may cause difficulties for some people, particularly given the current economic situation.
31. Mr Easton: As you know, I support a Bill for autism. I am not having a go at you, but I am a wee bit disappointed that it has been watered down, although, to an extent, I understand why. Was it watered down to heal the relationship with the Department, which was unhappy at the prospect of an autism Bill?
32. I am pleased that the Departments will be forced to work together to come up with strategies. However, I am disappointed that extra funding may not be forthcoming from those Departments, because I believed that we would force them to contribute. Therefore, although I am happy that the Departments will work together, I am disappointed that there will be no additional funding and that the advocate idea will not be progressed. Nevertheless, I will continue to support you.
33. Mr D Bradley: To a large extent, I share your disappointment. The dilution or watering down of the draft Bill was not a result of interaction with or feedback from the Department. We took the temperature of some of the parties, and the feedback was that resource implications might make it difficult to move the legislation through the Assembly should it include the position of advocate or commissioner. We thought that such an inclusion would, perhaps, lead to the proposed Bill's not becoming an Act. Although we regretted doing so, we had to balance one element against another, and, with the support of the all-party group, we decided that it would be better to progress the key elements of the legislation and that the advocate's position should be held in reserve for the future.
34. Mr Easton: I suppose that it is better to bank what we can now and work towards achieving more later.
35. Mrs O'Neill: As you know, I strongly support an autism Bill. When the Committee wrote to the Office of the First Minister and deputy First Minister (OFMDFM) about changing the DDA to include social communication disability, its response was that there was no need to do so. Looking ahead to the Committee's scrutiny of the legislation, I assume that officials of OFMDFM and the Health Department will attend as witnesses. Will you explain why the DDA needs to be changed and why people with a social communication disability are not protected by it at present?
36. Mr D Bradley: One practical reason is that Departments use the DDA as guidance when, for example, awarding disability living allowance. Consequently, people with autism have not benefited from the guidance. Arlene will expand on that point.
37. Mrs Cassidy: I have a list of issues that may be useful in helping people to get their heads round the implications of amending the DDA. The systematic education of the public that would flow from the adaptations to public spaces and facilities; the emotional hook of ASD being recognised in law would bring a level of validity regarding a condition that is still treated with suspicion and ignorance by some professionals and agencies; and clarity in law is a practical benefit that would guide decision-making on benefit entitlement. I will elaborate on the third point: some DLA adjudicators have disallowed benefits because a child's condition of autism did not fit with the definition of disability that appears in the DDA. We can present such decisions as evidence in support of our case. Such legal clarification will also lead to the updating of disability action plans for public bodies and an improvement in access to equality legislation. Families will have a reference point for entitlement to services, such as those for people with autism whose IQ has been assessed as 70 or above. Finally, the physical adaptations to public buildings will assist not only those with ASD but the wider disabled community.
38. Mrs O'Neill: I am on board with the change to the DDA. I thought that it would be useful for the Committee also to be aware of the implications, because we will have to deal with the counter-arguments. The fact that a commissioner, or whoever was involved in the tribunal process, refused someone a benefit because autism did not fit is a powerful argument and just what we need to drive through the legislation. You mentioned that you have evidence of such cases. It would be great if you could provide that to the Committee.
39. Another issue is that the Health Department might say that it already has a strategy in place. Will you comment on how your strategy will differ?
40. Mr D Bradley: The Department of Health, Social Services and Public Safety has an action plan on autism, and the Department of Education is formulating a strategy on autism. In a way, that illustrates the need for strategies to be streamlined between Departments. Indeed, some Departments that need such a strategy do not have one at all.
41. We welcome the Health Department's action plan. It can fit into and become part of the legislation. The draft Bill does not negate that action plan, but encourages its integration with strategies in other Departments. In that way, the services that people with autism receive can be streamlined between Departments and between the various transitional stages of their lives.
42. Mrs Cassidy: I noted a few points that might be helpful to the Committee. By recognising in law the requirement for cross-departmental planning, buy-in and synchronicity, an autism Bill will make a real difference to families. As Dominic indicated, the strategy will assure families that government recognise the lifelong and whole-life reality of autism. Through shared funding initiatives across Departments, it also assures the potential for service development during harsh economic times. The strategy identifies autism is a shared responsibility in our community. It means that duplication and confusion can be addressed and transitions, which are uniquely distressing for individuals with autism, can be better planned and resourced.
43. The Chairperson: I may be playing devil's advocate again, but why do other conditions, which are sometimes complex and have implications that cross several Department, not demand a similar Bill and treatment?
44. Mr D Bradley: Perhaps some of them do. The Department of Health, Social Services and Public Safety considers that autism requires an action plan. Indeed, it has formulated such an action plan and set up original reference groups to deal with that. That Department agrees that there is a need to focus on autism and to undo its history of neglect. The Department of Education also set up a task force on autism, yet it did not establish a task force on any other disorder or disability. It is also formulating a strategy on autism and agrees that action must be taken to tackle the ignorance that surrounds autism and to undo its historical neglect.
45. The Health Department and others argued that it was wrong to focus on one particular disorder or disability. However, both the Health and Education Departments have adopted a focus on autism.
46. Mr McCallister: My question about the potential risk was on the same lines as that of the Chairperson. Given your reply to the Chairperson, is there any risk involved in having an autism Bill? The Health Department has, for example a stroke strategy, but we do not legislate for that. I also have concerns about autism and any sort of special need that is difficult to identify in young children. I have dealt with some statementing issues in my constituency. Will legislation take autism to a level at which it is almost advantageous for a child to have had the condition diagnosed when attempting to acquire a statement of educational need? Do you regard that as a risk inherent in setting autism on a different level from other conditions or needs?
47. Mr D Bradley: No. You described a scenario in which parents might regard a diagnosis of autism as a means of obtaining a statement of educational need. I do not consider that to be a danger connected to the legislation. Most parents to whom I have spoken, and I am sure that you have spoken to many in your constituency office, do not rejoice when their child receive a diagnosis of autism. In fact, some of them go into denial. Parents say that they wish that their child did not have autism and had been diagnosed with a less challenging condition. No parent wants a child to receive an inaccurate or irrelevant diagnosis of autism. Based on our evidence of parents' reaction to such a diagnosis, that is not the case.
48. Mrs Cassidy: That goes back to the core issue of an autism Bill, which is the amendment to the Disability Discrimination Act. The current definition refers to disability as physical or mental, and, under the latter, to learning disability and mental illness. As autism is none of the above per se, but can be any of the above, it is not included. As I said earlier, much flows from its non-inclusion. That is a fundamental flaw in our system, and we hope that other equalities will flow from its redress to afford autism equality with other disabilities. We want equality for autism, not for it to be regarded as something special or above other conditions.
49. Mr McCallister: If I may widen the scope, autism is a developmental illness that does not fit neatly into any category.
50. Mrs Cassidy: As you know, autism involves social and communication impairment, and the intention is to include wording to reflect that in the amendment to the DDA. There is a precedent for the DDA being amended, as it was to include conditions such as cancer and HIV. We are bringing the DDA up to date to make it relevant to today and to what we know about autism.
51. Dr Deeny: I have a couple of questions, the answers to which might not be a simple yes or no. Does autism require a specific Bill? The Chairperson asked why we should not have specific Bills for other conditions. Is legislation for autism required because of the problems that have arisen from it not falling directly under a single remit but crossing the remits of health and education?
52. Arlene, GPs see a wide range of ASD in their practices. A couple of patients in my practice are highly autistic, and it would take a specialist to tell that others are autistic at all. Is the width of the spectrum a problem?
53. You mentioned that people with autism who have a high IQ are excluded from gateway services.
54. Mrs Cassidy: The issue of the IQ level is a current one. The situation is that a child with autism who has a co-existing learning disability can access services through the learning disability services. Children with autism who do not have a learning disability cannot access child and adolescent mental health services (CAMHS) if their IQ is 70 or above, unless they have a co-existing mental illness. The Southern Trust has made some strides in that respect, but I know from parents' experiences in many other trusts, an IQ of 70 or below was required to access the gateway to services.
55. Dr Deeny: Does an IQ of above 70 exclude children from access to those services?
56. Mrs Cassidy: Yes.
57. Dr Deeny: Does that tie in with the severity of ASD? Some people with autism are severely affected, and, in many cases, their IQ cannot even be assessed.
58. Mrs Cassidy: I can give only my perspective. As recently as 15 years ago, many people believed that someone with autism also had a learning disability. The statistics were that 75% of people with autism had a learning disability and 25% did not. We now know that the true position is exactly the reverse, and we have a better understanding of what life is like for those individuals who have an IQ of above 70. Many people consider that those with an IQ of above 70 cope better, but their families have to deal with a different set of severe difficulties.
59. In answer to your other question, the width of the autistic spectrum has become an issue as our understanding has grown over the years. An autism Bill aims to bring us up to speed. Our knowledge of autism and its prevalence have shot through the roof. The current system is creaking in an attempt to meet the accelerating need. The legislation aims to create a foundation on which we can build.
60. Mr Gallagher: I support the draft Bill and acknowledge the work that has gone into it. We are trying to achieve a seven-year strategy that will be published by the Department. The idea is that the trusts will feed into the strategy and provide the resulting data to the Department. Arlene, you said that autism rates are rising and rising. Do you envisage the trust providing that data every seven years or annually? Have you decided on that yet? Everyone agrees that the rate of autism is rising? Have you considered whether that data should be collected by the trusts every seven years, or should that be done every year so that the Department has the up-to-date data on its desk?
61. Mrs Cassidy: Data collection for planning purposes has to be done annually. The education and library boards collect data on school-age children with autism. A couple of weeks ago, at an event here, a colleague from the Belfast Education and Library Board told me that the prevalence rates that Autism NI was quoting, of one in a hundred, were out of date. I said that I knew that they were conservative but that we did not want to send out the message that the condition is more prevalent than it is. He quoted a rate of one in fifty in Northern Ireland, and we are now seeking to confirm that.
62. The cross-departmental issue of data collection in the draft Bill focuses more on synchronising the data collection of the Health and Education Departments. The Department of Education has a track record in data collection, but the Department of Health, Social Services and Public Safety has not and is addressing that in its action plan. I cannot report to the Committee on how far that work has progressed, but data collection has been flagged as an issue. The aim is to synchronise such effort to improve cross-departmental planning.
63. Mr D Bradley: If Tommy was suggesting that it would be useful for information to be updated much more regularly, I agree. It is hoped that the strategy will not remain static over the seven years, but that it will be sensitive and adjusted in response to information fed back from the statistical report.
64. The Chairperson: Any autism Bill will undergo a Committee Stage, so we will have plenty of opportunity to scrutinise it then.
65. Thank you very much, Dominic and Arlene, for your evidence. The Committee will probably see a great deal of you in connection with the legislation over the next few weeks and months.
66. Mr D Bradley: I thank the Chairperson and Committee members for engaging with us today. Although some of the points raised were quite challenging, they were useful and constructive. They will be helpful to us as our work on the draft Bill continues.
2 December 2010
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mr Pól Callaghan
Mr Alex Easton
Mr Tommy Gallagher
Mr Sam Gardiner
Mr Paul Girvan
Mr John McCallister
Witnesses:
|
Dr Maura Briscoe |
Department of Health, Social Services and Public Safety |
67. The Chairperson (Mr Wells): We have with us representatives of the Department of Health, Social Services and Public Safety. Some of the faces will be familiar to the Committee. Dr Maura Briscoe is the mental health and disability policy director, and has been before us on several occasions to address various issues; Dr Ian McMaster is a medical officer in the Department; Dr Hilary Harrison is a social services officer in the Department; and Peter Deazley is from the Department's learning disability unit. Please give the Committee a 10-minute presentation on the Department's position on the Bill.
68. Dr Maura Briscoe (Department of Health, Social Services and Public Safety): Thank you very much, Mr Wells. Good afternoon, everyone. We fully recognise the importance of autism. We have, through various mechanisms in the Department, tried to promote and enhance autism services for children and adults, particularly over the past few years, and we will continue to do so. Therefore, on that basis, we believe that legislation is unnecessary at this time. I will drill down into the detail of why we think that it is unnecessary. Before I do that, however, I highlight that there has been substantial investment over the last comprehensive spending review (CSR) period. There have been a number of successes, including the formation of the regional autism spectrum disorder (ASD) network group, a significant reduction in waiting times for children for assessment and diagnosis, and the launch of a children and young people's assessment and diagnostic care pathway. The Committee will have heard the recent announcement about investment in adult autism services.
69. I do not propose to go into the detail of service provision. Rather, I will concentrate on the legislation and why the Department does not support it at this time. Members will see that the Autism Bill seeks to unilaterally change the Disability Discrimination Act 1995 (DDA) to include terms such as "social interaction (including communication)" and "social relationships". As the Committee knows, England has an Autism Act and a Bill is proceeding through the Scottish Parliament. No other jurisdiction has sought to change the UK/Westminster-enacted legislation to put in place a very broad definition in the Disability Discrimination Act.
70. Members will have seen the Office of the First Minister and deputy First Minister (OFMDFM) guidance for Northern Ireland on the Disability Discrimination Act. It is quite clear, and there are specific examples under DDA on autism. That is supplemented by recent case law that makes clear that autism is covered by the Disability Discrimination Act. It is unclear why the very broad definition of "significant difficulty" as:
"(i) taking part in normal interaction; or
(j) forming social relationships"
71. is being proposed to amend UK-wide legislation unilaterally in Northern Ireland. Clearly, there is a cost in doing that in respect of legal opinion, consultation, and reissuing and redeveloping guidance. There may also be challenges from individuals, for example in relation to workplaces or schools, etc, with a resultant potential cost. Given that there is already clear guidance, it is unclear why there is a proposed unilateral change in definition in the DDA.
72. The Bill also seeks to change the definition of autism. Members will note that no other UK jurisdiction has sought to define autism in primary legislation. Indeed, the Committee will have noted that Scotland considered it disadvantageous to do that because research and understanding of autism and the range of the spectrum will change over time. Therefore, that was not put in legislation. In addition, the inclusion of any pervasive disorder that is not otherwise specified in the legislation would have the potential to widen the scope of autism and, therefore, may include individuals who would not generally be considered to have autism. That may, over time, have an impact on prevalence data and the labelling of individuals with autism.
73. One of the main provisions of the Bill relates to the autism strategy. That is not in any other legislation, it is an indefinite autism strategy, and it is mandatory. That would place the Health Department in the lead position in respect of the future production on an indefinite basis of an autism strategy. Minister McGimpsey made it clear that he does not need legislation to effect change and improve ASD services. Indeed, a new strategy with a new bureaucratic infrastructure to monitor it could slow down progress in moving forward with our enhancements for ASD services.
74. Members will also note that the Department of Education is producing an autism strategy for consultation in the new year. Therefore, there is potential for confusion with the new autism strategy as defined in legislation.
75. We already have a DHSSPS autism strategy, we already have a multidisciplinary ASD regional network group, we already have a reference group that includes 30 parents, carers and service users, along with 10 voluntary organisations. The implementation of the English strategy is not a million miles away from the infrastructure that we had ahead of them.
76. The Bill also states that DHSSPS will be the lead Department responsible for monitoring all other Departments that are required to contribute to the implementation of the strategy. No other jurisdiction has that in its potential legislation. Indeed, the recent Scottish legislation mentions Scottish Ministers — plural.
77. We feel that all of that will involve bureaucracy. The requirement to monitor the rolling indefinite nature of the strategy will cost money that we feel would be better placed in front line service provision. The Bill also asks us to collect prevalence data, but we have already recognised the need to do that. We do not need legislation for that. Members will note that the recent launch of the children's care pathway on assessment and diagnosis is one step in the general direction to ensure streamlining of those services and enhanced data collection.
78. Finally, there is no detail on resources in the financial memorandum, but we feel that costs will arise from a cross-departmental strategy, the consultation process, extensive monitoring arrangements to be put in place, unilateral amendment to the DDA and from potential challenges that might ensue from those changes. Clearly, further guidance will need to be developed on the DDA. Costs will also stem from a public information campaign and to rolling out training for front line civil servants in all Departments. There will be a cost to implementing the actions in the new strategy, and that is not addressed. We would far prefer to see costs and finances going to front line services.
79. In summary, with the combination of the unilateral amendment to the DDA, a wider definition of autism, the costs and bureaucracy associated with the Bill, and the monitoring arrangements that would need to be put in place, we would far prefer to concentrate on areas where we are moving forward in partnership with what has already commenced through the regional ASD network group to improve front line services. Therefore, the Department believes that the legislation is unnecessary.
80. The Chairperson: Thank you, Dr Briscoe. On a procedural point, I may have to nip out at some point, because there is some interest in the issue of waiting lists. The Deputy Chairperson is not here, so we will have to go through the procedure of nominating an acting Chairperson. Do we have any nominations for acting Chairperson?
81. Mr Gardiner: Mr Easton.
82. The Chairperson: Mr Easton will assume that role, as usual.
83. Dr Briscoe, you made the point that, because the rest of the UK does not have such legislation, we should not have it. The view that many people would take is that we in Northern Ireland should be trailblazing, leading from the front, and trying to do our best for our autistic children. Others have not had the pioneering spirit to do this, but does that mean that we should automatically or slavishly agree with them?
84. Dr Briscoe: Not at all. We are potentially ahead of other jurisdictions in having had an ASD network group in place and a strategy in 2009, before England put through its legislation or Scotland initiated its legislation. I emphasise that broad definitions such as "social relationships" and "including communication" will have knock-on effects that will be unilateral to Northern Ireland. They may potentially cause significance, perhaps not this year, but further down the line. Do not forget that the wording is not related to autism, but to broad words such as "social interaction" and "communication", so it has the potential to widen the net.
85. The Chairperson: Autism groups have made the point that, at present, the definition of disability in Northern Ireland, physical and mental, does not necessarily cover every autistic child. The child might be all right physically and be very bright, but have enormous problems.
86. Dr Briscoe: I am happy to accept that point. I refer you to the OFMDFM guidance on the Disability Discrimination Act 1995, which clearly defines disability in the context of impairment. It specifically says that:
"It is important to remember that not all impairments are readily identifiable."
87. It goes on to list a range of them, including:
"learning or developmental difficulties such as autism spectrum disorders, developmental co-ordination disorders or dyslexia".
88. If you read through that guidance, you will see that there are at least two specific examples in relation to autism spectrum disorder. There is also case law that does not support the view that autism is not covered by the Disability Discrimination Act 1995.
89. The Chairperson: I have been familiar with these processes for 30 years, Dr Briscoe. I know that there is a world of difference between a definition in legislation, and one in guidance. In legislation, a definition allows a parent to take a judicial review or court action if he or she feels that a child has not been properly dealt with. Guidance is simply that. Therefore, it much more powerful to have a specific reference in legislation that defines what is meant by an autistic child.
90. Dr Briscoe: "Social interaction" and "communication" do not define what is meant by an autistic child. I draw your attention to the fact that there is case law that clearly identifies that ASD is recognised as a disability under the Disability Discrimination Act 1995.
91. The Chairperson: Parents tell me that inclusion of the word "social" will guarantee that every child in the autistic spectrum will be covered. It is unusual condition: a child could be like Linford Christie with respect to his physical attributes. Some of those children are incredibly intelligent, and the ability of some of those people in maths and drawing is phenomenal but, because of their social abilities, they are different and they have problems in interacting with other children and their peers. That word guarantees that they will be covered. It ensures that no child will fall between two stools. That is what the parents are looking for.
92. Dr Briscoe: If you look at the categories in the Disability Discrimination Act 1995, under schedule 2(4), it includes mobility, manual dexterity, physical co-ordination, constant ability to lift, carry or otherwise move everyday objects, speech, hearing, eyesight, memory or ability to concentrate, learn or understand, or perception of the risk of physical danger. This Bill will add underneath that the words in regard to social relationships, and so on. Therefore, only one of those categories needs to pertain, and that opens up the Disability Discrimination Act 1995 potentially much wider than was intended in the Autism Bill.
93. The Chairperson: Some children will tick all of those boxes, but they will still have incredible difficulty interacting with their peers.
94. Dr Briscoe: I draw attention to the fact that that is already covered in the guidance under:
"memory or ability to concentrate, learn or understand".
95. It gives as an example:
"significant difficulty taking part in normal social interaction or forming social relationships".
96. If there is case law and, within the definition of DDA, not only here, but across the water —
97. The Chairperson: It is in the guidance and the case law. Why not beef it up and make it perfectly clear by enshrining it in legislation?
98. Dr Briscoe: That would expand the category much wider than autism and would have potential knock-on effects with regard to protections under the DDA for a range of conditions. There are lots of conditions beyond autism that involve social impairment and social interaction. Can you imagine what that could mean in the workplace if somebody said that his or her difficulties with social interaction and social relationships impaired his or her day-to-day activities?
99. The Chairperson: It could mean that those people's difficulties might be covered by the DDA. I am merely putting the points that have been made to me. Alex Easton will take over the Chair; I will be back in five minutes. I know that members are keen to ask questions on this issue.
(The Acting Chairperson [Mr Easton] in the Chair)
100. The Acting Chairperson (Mr Easton): Does any member wish to ask a question?
101. Mr McCallister: I have a continuing concern about the Bill as it is drafted. We know that the Department of Health, Social Services and Public Safety has a strategy up and running, and you have said that this Bill could slow down the implementation of that strategy. How far along the track are you with the strategy? How much will it be slowed down? The Department of Education is going to take forward a strategy. There is a Department of Health, Social Services and Public Safety strategy and a Department of Education strategy, a plank of which is the centre at Middletown. There is a fair divergence of opinion between the Departments. How will the Bill overcome and deal with the differing strategies of the two Departments?
102. Dr Briscoe: There is a good working relationship in the regional ASD network group between the two Departments. At local level, the regional group comprises people involved in education, and the chairperson of the ASD network, Dr Stephen Bergin, is a member of the education and library boards' inter-board ASD group. There is a good working relationship. I am not here to talk about the Department of Education's ASD strategy; I have no idea what is in it. I cannot talk about that. Our prevalence data on children and the sharing of information will be checked against any prevalence data held in the Department of Education.
103. Therefore we see, again, that on the ground there is already partnership working between health and education at all levels, so having a strategy in legislation is not going to make any difference.
104. What I mean by slowing it down is that we are well advanced in our strategy. There is an annual report on our strategy, which is one of the things that would be required by the Bill — we are already doing it. Our quarterly monitoring reports against the trusts' performances as part of our ASD action plan are also well advanced. The children's care pathway is a major piece of work that has the potential to streamline assessment and diagnosis — the tools that will make the collation of data and services much more effective.
105. We do not wish to see a dismantling of the regional ASD network group, which new bureaucratic monitoring systems that involve all Departments would clearly bring about. We are holding workshops in the new year to start evaluating our ASD strategy, which will then be rolled forward. Anything that cuts across that is going to slow us down.
106. Mr McCallister: If the Bill goes through and you are the lead Department, what happens if the other Department disagrees with what you want to do? Who gets priority? If the Department of Education decided to stick with the Middletown centre, for example, and the Department of Health said that it was a white elephant or a waste of money, how would you make those two different opinions meet? It is encouraging that you have outlined a good relationship between the Departments which are both so intricately involved, but I do not know what would happen were policy to go off in two different directions.
107. Dr Briscoe: The Department of Health would be required to monitor the actions of other Departments.
108. Mr McCallister: So, you would have to monitor —
109. Dr Briscoe: Any actions in the strategy attributed to other Government Departments, they would have to implement. In Scotland, they talk about Scottish Ministers rather than one lead Department. The implication of monitoring is that we would monitor all other Departments, and the Bill requires other Departments to implement their aspects of the strategy. Therefore, the strategy would follow due process by going out to consultation and so on. That is the basis on which the final strategy would be agreed.
110. Mr McCallister: Would your Department's monitoring include reporting back on whether it thought that a strategy was wrong or ineffective? Potentially, might you report that back without making any difference to it?
111. Dr Briscoe: We would report as fact what other Departments were doing.
112. Mr McCallister: But possibly could not do anything about it?
113. Dr Briscoe: The strategy would be consulted on in advance. Therefore, whatever the outcome of that consultation, Executive agreement would be needed to publish the strategy. It would be up to the Executive to publish it. The decision on the content of the strategy would be an Executive decision, not one for one Department. We would have to monitor, post-consultation, once the Executive agreed the final strategy.
114. Mr McCallister: But that could deadlock the strategy. You might end up with nothing being done.
115. Dr Briscoe: That is why, as I say, we do not want a new strategy to cut across the good work that the regional ASD group is doing. Through that network group, we will be holding workshops in January and February in relation to rolling forward our 2009-2011 strategy.
116. I again emphasise that on the ground, at regional and local level, the interface with education is good and there is an interrelationship there that can and is being built on through participation in its ASD group and our ASD group. Given that the final strategy is a cross-departmental strategy, I imagine that it would be for the Executive to agree to its publication.
117. Mr Gallagher: It seems to me, unless you can convince me otherwise, that you are just concerned with limiting the autism strategy to your Department's view of it. You are not giving consideration to the wider lifetime needs of individuals who suffer from the condition.
118. We are talking about legislation. While you can be effusive about guidelines, parents are very angry and annoyed about the failure of the system and of those guidelines. The needs of their children are not being met. Parents are very worried that, as their children move into adulthood, their needs are not being met. The Bill is designed to meet those needs. Why would you not agree that:
"The autism strategy must set out how the needs of persons with autism are to be addressed throughout their lives ... the needs to be set out in the autism strategy shall include the health care, educational and social needs of persons with autism … The autism strategy must set out how the needs of families and carers of persons with autism are to be addressed"?
119. How can you convince me that that is not an improvement on the current situation?
120. Dr Briscoe: I am sure that you have read our autism strategy and strategic action plan. Within that strategy, actions are listed under five key themes: service redesign to improve ASD care; performance improvement in ASD services; training and raising awareness; communication and information for individuals and families; and effective engagement and partnership working. As we move forward with the action plan we will be able to address, through those themes, the issues that you have highlighted. We emphasise again that we do not feel that we need legislation to do that.
121. The first annual report of the regional ASD network group specifically says that it is taking a life cycle approach. You will have noted that the investment recently announced by Minister McGimpsey for transitions and adult autism services is in recognition of the fact that autism services are about a lifelong approach. We believe that we have the infrastructure to build on to be able to do that.
122. As you will appreciate, this is a relatively new arrangement with both the ASD action plan and the regional group. Therefore, yes, our concentration to date has been in our own backyard in trying to reduce waiting times and get a children's care pathway in place. However, that children's care pathway very much identifies family support, the crossover into education and the production of care plans, which include all the aspects that you talked about. We do not feel that legislation is required to do that.
123. Mr Callaghan: Good evening. In case any of you do not know, I am Pól Callaghan, the new SDLP Member for Foyle replacing Mark Durkan.
124. A few things came up in what was a very interesting presentation, Dr Briscoe.
125. Dr Briscoe: Thank you.
126. Mr Callaghan: The topic is obviously very important to not just everybody in the room but to the wider autism community. We all know that that community has a very genuine concern and interest in all of this. I will go step by step through this so that I do not get lost.
127. You seem to be bringing up the matter of judicial interpretation in relation to clause 1(3), the stuff about:
"taking part in normal social interaction; or … forming social relationships."
128. Maybe I am getting the wrong end of the stick, but it seems to me that you are somehow implying that, in a judicial action, that may be interpreted as referring to a '40-Year-Old Virgin', as the film has it, who cannot chat up a girl in a disco. However, if a case went to court, any judge looking at that clause would clearly understand that, in the context of the Bill, certain specific conditions fall within the autistic spectrum definition. Do you not accept that view?
129. Dr Briscoe: No.
130. Mr Callaghan: On what basis do you not accept it? Is there any case law to demonstrate that any judge would go beyond the context of a Bill, which, in this case, is specifically cited as an Autism Bill?
131. Dr Briscoe: The amendment is to the DDA and does not specify autism. Therefore, all that will be included in the DDA is "social relationships", with no reference being made to autism.
132. Mr Callaghan: I am not a lawyer, but, you know, if you read what judges say in case law history, you see that judges give regard to the context of the Bill. This Bill going through this legislature clearly states that it is to be referred to as the Autism Act and specifies autistic conditions. What it is that you are afraid will be trapped within the scope of the Bill? I do not really understand. I am not being flippant or frivolous for a second; I am absolutely serious. Is the Department suggesting that some guy who is too shy to chat up a girl or a guy in a disco could take an action under the DDA using that instrument? Is that what you are seriously suggesting? If not, I do not understand what it is that you are suggesting.
133. Dr Briscoe: As you say, this is not a frivolous matter. You have listed a very extreme example of social relationships. One needs to go back to the definition in the DDA of "impairment" — a definition that would also cover any changes as outlined in this Bill — as something that has a significant adverse effect on a person's ability to carry out normal day-to-day activities. Given that the purpose of the DDA is to give extra protection to those who have impairments that have an adverse effect on normal day-to-day activities, regardless of the cause of those impairments, your example is neither here nor there.
134. You mentioned the judiciary and case law. I say to you that there is already case law that clearly says that ASD is covered by the Disability Discrimination Act 1995. Therefore, we have to ask why it is necessary, on those grounds, to put in generic wording such as "social relationships" when it covers a broad range of conditions, not just autism. The add-on to the 1995 Act will be about social relationships, but there will be nothing on autism.
135. Mr Callaghan: I am not sure that that is so. There is a clause in the Bill specifically about interpretation and, clearly, interpretation is what is at issue. If someone comes before a court arguing that their case be included under the DDA on the basis of this Bill, if it were passed by the House, and some condition that is not diagnosed as autism or one of the other specified conditions — Heller's or whatever else — a judge would have to give regard to the interpretative provisions of the Bill. The one does not stand without the other, or perhaps I am missing something.
136. Dr Briscoe: The Bill amends specific clauses and schedules in the DDA. The Bill talks specifically about social interaction and social relationships —
137. Mr Callaghan: I understand that. However, my point is that there are other provisions in the Bill that are, effectively, statutory interpretive guidelines for the judiciary. It seems to me that the Department's presentation today has no regard to those provisions in the Bill.
138. Dr Briscoe: I am not sure that I understand what it is that you are saying. I reiterate that, from the Department's perspective, it is clear in the official guidance underpinning the DDA and in case law that autism is already included in the DDA. Given that that is the case, we ask the Committee why it is that one would need to include that broader definition.
139. I want to move on, because you asked quite important questions about the definition of "autism". We have other concerns about the definition, and my colleague Dr Ian McMaster will talk about that important definition and its potential consequences.
140. Mr Callaghan: I am happy for Mr McMaster to come in on that point, but I do have further questions for the Department.
141. The Acting Chairperson: How many questions?
142. Mr Callaghan: Probably four.
143. The Acting Chairperson: Can you do them all in one go?
144. Mr Callaghan: That depends on the response from the Department.
145. The Acting Chairperson: Try it; go for it.
146. Mr Callaghan: OK.
147. Dr Briscoe: Let me just say that the top bit — clause 1 — is an amendment to the DDA, as opposed to what is labelled the autism strategy, in which the definitions of "autism" are included. We see the top bit, which relates to the DDA, as potentially different from the autism strategy.
148. Mr Callaghan: I am not sure that I accept that. However, we will move on, because we have exhausted the issue.
149. Mr Peter Deazley (Department of Health, Social Services and Public Safety): Once the first amendment has been passed, the impact of the Bill will cease to exist. The DDA will then stand on its own, as amended.
150. Mr Callaghan: Yes, but it seems to me that the Department is blind to all the clauses in the Bill beyond the first clause.
151. Mr Deazley: No, but at the minute we are talking only about the clause that amends the DDA.
152. Mr Callaghan: The Committee is talking about the whole Bill.
153. Dr Briscoe: That is why we want to get on to the definition of "autism".
154. Mr Gallagher: We are talking about the definition of "autism".
155. Dr Briscoe: We are not. We are talking about the first clause, which amends the Disability Discrimination Act 1995.
156. Dr Hilary Harrison (Department of Health, Social Services and Public Safety): When the amendment to the 1995 Act is made, the fact that it has been amended as a consequence of the Autism Bill will have no bearing whatsoever on the interpretation of "disability" within the 1995 Act. For example, it would not mean that an employment tribunal looking at the social relationship aspect of discrimination would link that back to autism; it would link that back to any condition that involves poor social relationships.
157. Mr Callaghan: I am not sure whether that is a commonly held view; however, I understand your point.
158. Dr Harrison: Once the 1995 Act is amended, it will be completely divorced from the Autism Bill.
159. Dr Briscoe: Your other point about the definition of "autism" is also important, not in the context of the DDA but in the context of the broader Bill.
160. Dr Ian McMaster (Department of Health, Social Services and Public Safety): Effectively, although it is defined under clear syndromes that are recognised in the International Classification of Diseases, there is, nevertheless, a risk that diagnosis is not accurate in all cases. The classification shows a significant number of similar conditions that could be differential diagnoses for autism — Asperger's, in particular, and some of the other pervasive developmental disorders. Therefore, we have some concerns that people who are not intended to be picked up by the legislation, but who may have similar conditions, will be included. As this is a very emotive area and diagnosis, for parents in particular, there is an issue that people who do not fit the category could be labelled with the disorder.
(The Chairperson [Mr Wells] in the Chair)
161. The other concern relates to a point that was raised by Maura. As time goes on it is likely that autistic spectrum disorder will evolve and that there will perhaps be a change in view as to what is and is not included. Conversely, a tight definition might exclude some people with very similar needs who should be included in that.
162. The final point is that, as the Chairperson pointed out, it is the needs of the children or adults with autism that we should be focusing on, rather than spending time trying to assess and attach a specific category or diagnosis. Clinicians focus more on that, and the care pathway that has been developed for children and young people focuses very much on the initial triage and on the use of a standardised, approved, accredited method of assessment and diagnosis before taking parents and carers through that diagnostic labelling.
163. The Chairperson: Pól, are you happy with that?
164. Mr Callaghan: Sorry, Chairperson, I was not sure whether I was still asking questions.
165. You may have lost me on that point, Mr McMaster. In my view, the fact that clause 4(1) extends the scope of the Bill to include "any pervasive developmental disorder" means that, in the spirit of the Bill, the particular definitions of one condition or another are not really the issue. The focus of the Bill is not on determining whether or not someone is trapped like a mouse by the definition of "autism". The purpose of the Bill is to be fairly broad in scope, as long as a condition is comparable to an autistic spectrum disorder. I do not follow the point that you are trying to make.
166. Dr McMaster: The definition is:
"any pervasive developmental disorder not otherwise specified".
167. That definition is a catch-all to pick up people who do not quite fit the pigeonhole but who perhaps have three of the four necessary criteria, and you are quite right to differentiate them. That is probably the best pigeonhole for those people to fit in. However, other people with emotional behavioural problems — I am thinking of people with moderate to severe learning disabilities — would fit criteria very similar to those of a pervasive development disorder and yet are a separate entity. People with Asperger's syndrome can have schizoid personality disorders and have considerable difficulties with social interaction, but their cognition and language may be reasonable. Unfortunately, those people could be incorporated under that diagnosis. Diagnosis is not always accurate, particularly in this field where there are no specific tests that can be done.
168. Dr Briscoe: That is why, in Scotland, they specifically did not include a definition of "autism" on the face of the primary legislation. Over time, as Ian said, having a definition on the face of primary legislation might impact on the collection of prevalence data down the line. You can see that there are relatively small numbers. Nonetheless, that might, depending on what way you look at it, impact on the data collection and the prevalence data.
169. Mr Callaghan: That last point is probably more an observation than a basis for objection, is it?
170. Dr Briscoe: I am just saying that the Bill asks us to collect prevalence data on autism.
171. Mr Callaghan: It does.
172. Dr Briscoe: Clearly, we would have to link that to the definition of "autism" in the Bill.
173. Mr Callaghan: Absolutely. OK.
174. The Chairperson: Pól, you have had a very fair crack of the whip.
175. Mr Callaghan: To be fair, Chairperson, I am not sure whether that is the case. The Department took up much more of the time than I did.
176. The Chairperson: I think it was a case of when the cat was away, the mouse was playing a bit. I will let you back in at the end, but John has been waiting, and he is very sore.
177. Mr McCallister: I was in. It was related to Pól's point —
178. The Chairperson: Do you want to come in on this particular point, then?
179. Mr McCallister: If there is a rush to get in, I can wait until the end, but it was on that point. I put this point to the Bill's sponsor: if we define "autism" too tightly, will we have people with complex needs who will fall on one side of the line or the other? As Ian said, the diagnosis is not always very accurate. If families with complex needs have an autism diagnosis, that could open up a pathway to more than they have. Will that cause problems, or add to the problems of diagnosis in that if you get the diagnosis, you fall inside the scope of the Bill, and if you do not get the diagnosis, you fall outside it? In addition, will the prevalence lead to significant problems with the diagnosis? I am concerned that falling inside the scope of the Bill will create more of a problem.
180. Dr McMaster: It could change the emphasis from addressing the needs that you see in front of you to doing more extensive assessments to provide a diagnosis so that you can place people inside or outside the category. That in itself will divert clinical time and resources away from working on the needs of people.
181. Mr McCallister: How will that change over time if the definition is trapped in primary legislation, and there are developments over a five- or 10-year period? A strategy can obviously respond to that pretty much with a stroke of the Minister's pen, but you cannot do that with this Bill.
182. Dr Briscoe: You would have to amend the primary legislation to encompass it as research and development goes ahead and the definition of ASD potentially widens or narrows, depending on the direction of travel. Given that it is in the primary legislation, you would have to amend the primary legislation.
183. Mr McCallister: If the definition widened, for example, we could potentially end up excluding people six years from now.
184. Dr Briscoe: If research, the evidence base, and authoritative things such as the National Institute for Health and Clinical Excellence produced a definition of "autism" that was very different from that in the Bill, you would have to go back and amend the legislation.
185. Mr Gallagher: Do you accept that the Bill is enabling legislation?
186. Dr Briscoe: Just define what you mean by "enabling".
187. Mr Gallagher: That there are fine details that will be worked out once the Bill is passed.
188. Dr Briscoe: That is beyond the viewpoints that are in the legislation on the strategy. A lot of detail in respect of the strategy will have to be worked out. However, the Bill is not enabling in the sense that where we are going at the moment without legislation is also enabling.
189. Mr Gallagher: Ian reflected your concern that the legislation would be too inclusive and that people might be stigmatised as a result.
190. Dr Briscoe: It could be too broad.
191. Mr Gallagher: In other words, it is too broad and too wide.
192. Our view is that the existing legislation is too narrow. If it is accepted that it is enabling legislation, is it not the case that that can be worked out after the legislation is passed?
193. Dr Briscoe: No; not the definition. The definition is very clear. As I said, if the definition through, say, research —
194. Mr Gallagher: Will you give me an example of what you mean by "very clear"?
195. Dr Briscoe: The definition of autism is very specific within the strategy. If, for example, in three, five or seven years' time, new research evidence states that the cause of autism is X, and, therefore, the definition moves, clearly one would have to look at the primary legislation because there would need to be a link between the requirement to collect prevalence data and the definition of autism in the Bill.
196. Mr Gallagher: That applies to everything in life. That is why we change and amend legislation.
197. Dr Briscoe: That is why the other jurisdictions did not include a definition in legislation. They were happy to put that in potential guidance that could be easily changed but not in the legislation.
198. Mr Callaghan: We all appreciate that this is a complex matter. The Department of Health, Social Services and Public Safety would be, more or less, designated as the lead Department, with a co-ordinating role between Departments in implementing the strategy. I found it interesting, Dr Briscoe, that you said that you have no idea what is in the Department of Education's strategy.
199. Dr Briscoe: That Department has not yet published its strategy for consultation.
200. Mr Callaghan: That is not a criticism of you personally. However, I would have thought that one purpose of the Bill is to ensure that Departments are working together from the off to provide an overarching strategy that meets all the needs of people with autism and their families and that every Department is, therefore, held to account for its actions.
201. John asked what you could do if your reports showed that one Department or another was not fulfilling its obligations under the strategy or whether that would make no difference. The difference in respect of the Bill is that those Departments will be judicially reviewable for their failure. With respect, you keep referring to guidance and the existing strategy, but that is not a judicially reviewable sphere of operations, and that is absolutely core to the Bill.
202. My final point is about the wider purpose of the Bill. Unfortunately, we all know that when budgets are tight and financial pressures are hard, statutory agencies and Departments often first target matters that are not protected by statute. I support the Bill because it will provide statutory protection for autistic services in the future. Although the current Minister says that he is committed to an autism strategy, that is entirely at the discretion of the Minister of the day, whereas the law is not. The Department did not address that in its presentation.
203. Dr Briscoe: The Bill's explanatory and financial memorandum refers to the production of an autism strategy. It does not detail resources, and so forth, for that, so it would be for the Executive to approve a strategy.
204. The Department's role is about more than co-ordination. There is a role to monitor other Departments. It is quite unusual in legislation to have one Department monitoring other Departments. There is no detail in the explanatory and financial memorandum about an autism strategy because there is no cost attached to the strategy. Although in statute there would be an ASD strategy, there is, as I understand it, no protection in statute for the resources attached to that strategy.
205. Mr Callaghan: However, the Bill implements statutory duties, Dr Briscoe.
206. Dr Briscoe: There is a requirement to participate in a cross-governmental strategy, but —
207. Mr Callaghan: There are statutory duties on your Department, regardless of the explanatory and financial memorandum.
208. Dr Briscoe: Indeed, and we are working on our services for adults and children without any requirement for further legislation. In fact, we think that we have done considerably more than is potentially in the Bill.
209. Mr Deazley: The legislation makes it a statutory requirement to develop a strategy with co-operation and input from other Departments. Other Departments will develop a strategy for their services. We cannot tell them what improvements they have to make to their services. Eight or 10 component parts will be brought to the Executive for approval. Our role will be to monitor what other Departments say that they are going to do, not what we instruct them to do. We are legally obliged to have the strategy in place. The strategy must address how we are going to meet people's needs; it does not place any statutory obligation on us to actually meet those needs any more so than we do at present. We have a statutory requirement to meet needs as they emerge and to wrap those needs around a diagnosis. The money has to come from somewhere. If it is protected for one group of people, it must come from another group.
210. Dr Briscoe: I want to make it clear that the Bill does not require resources to be made available. It requires a strategy. The implications of that are, of course, that there is an expectation of resourcing, but there has been no analysis, and there is no statutory duty in that regard.
211. The Chairperson: I am conscious that if the Bill passes its Second Stage, we will be back here anyway, perhaps many times. We will have an opportunity to deal with anything that has been missed. This evidence session has been useful. At least you have set out clearly the Department's view, which is useful for folk who are considering which way to vote next week. Thank you very much.
212. Dr Briscoe: May I say one more thing, Mr Wells? I think that this dialogue has been very helpful, but I would like to end by reassuring the Committee, individuals, parents, carers and service users that the Department is absolutely committed to recognising the needs of people with autism and to doing its level best to promote and enhance services for autism for children and adults. We do not need legislation to do that.
213. The Chairperson: Thank you.
16 December 2010
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Mickey Brady
Mr Pól Callaghan
Dr Kieran Deeny
Mr Alex Easton
Mr Tommy Gallagher
Mr Paul Girvan
Mr John McCallister
Ms Sue Ramsey
Witnesses:
|
Mrs Fionnuala McAndrew |
Health and Social Care Board |
|
|
Dr Stephen Bergin |
Regional Autistic Spectrum Disorder Network |
214. The Chairperson (Mr Wells): Folks, I suggest that we structure our questioning of all witnesses, not only the current group, by dealing first with the proposed amendment to the Disability Discrimination Act (DDA) 1995, followed by the proposal for an autism strategy and, finally, a third set of questions on any other issues. If members are content, we will order our questions in those three stages.
215. I welcome the witnesses, all of whom have appeared before the Committee previously in some capacity. Mrs Fionnuala McAndrew is the director of social care and children's health at the Health and Social Care Board; Dr Stephen Bergin is the chairperson of the Regional Autistic Spectrum Disorder Network (RASDN) and a public health consultant with the Public Health Agency; and Mr Kieran McShane is the commissioning head of children and families at the Health and Social Care Board and network project team manager for the Regional Autistic Spectrum Disorder Network. Kieran, I believe that, a few months ago, you gave evidence to the Committee in the Senate Chamber. Is that correct?
216. Mr Kieran McShane (Regional Autistic Spectrum Disorder Network): That is correct.
217. The Chairperson: You have 10 minutes in which to make a presentation, after which the Committee will ask questions in three stages, as you heard.
218. Mrs Fionnuala McAndrew (Health and Social Care Board): Thank you, Chairperson, for the opportunity to make a presentation to the Committee this afternoon.
219. Reference has been made to the independent review of autism services. Committee members will be aware that, following publication of the regional action plan for autism, the implementation of recommendations in the report is being taken forward by the Health and Social Care Board through the Regional Autistic Spectrum Disorder Network (RASDN). The project structure for that network has been established under the leadership of Dr Stephen Bergin.
220. The RASDN project structure ensures a line of accountability from trust groups to a project board, which has representation at director level from the health and social care trusts; senior Health and Social Care Board officers; other statutory bodies; the Department of Education; the Department for Employment and Learning, and the Department for Social Development. It also has links with the criminal justice system. The project board is accountable to the Health and Social Care Board and, through the Department, to the Minister of Health, Social Services and Public Safety.
221. A fundamental and integral part of the network is the involvement and participation of the voluntary and community sector, parents, carers and service users at all levels in the project structure. At present, 10 voluntary and community sector organisations are involved in the reference group, which, as you know, is chaired by Lord Maginnis of Drumglass. They include groups such as Barnardo's, Autism NI, the National Autistic Society and Mencap, to name but a few. All those organisations can demonstrate active involvement in the design, planning and delivery of services to those with autistic spectrum disorder (ASD) and to their carers across children's and adults' services. They reflect the diversity of need. The predominant membership of the reference group, however, comprises parents, carers and service users. That is to ensure that those who are in direct receipt of services and who experience the realities of living with ASD have a voice in the planning, commissioning and evaluation of services. As part of the ongoing engagement, a series of stakeholder events has taken place across Northern Ireland. Those will continue as part of the project's infrastructure to ensure broad stakeholder involvement.
222. Given that the current membership of voluntary organisations involved with ASD represents a small proportion of the total users and carers who are impacted by it, the project seeks to ensure that it engages the hidden voices of the majority of those affected and that they have an opportunity to shape services.
223. Several work streams have been established within RASDN, including children and transitions; adults and transitions; training and awareness raising; and communication and information. If members wish to pursue the work of those work streams in their questioning, my colleagues will be happy to outline the work being taken forward.
224. We want to highlight some issues in connection with the need to enact additional and specific legislation. The DDA has already been referred to this afternoon, and I do not want to go over that ground, but we believe that that is all-encompassing. In addition, a number of clear statutory duties are outlined for trusts in the delivery of services to children with disabilities and their families, including those with autism. The Children Order 1995 is the primary legislation for children in Northern Ireland. Article 17 of the Order states:
"a child shall be taken to be in need if … he is disabled".
225. Article 18 of the Order determines the statutory responsibilities of trusts to provide services for children in need in their area. We are, therefore, required to consider those children determined to be in need by virtue of article 17. In addition, the Order imposes a statutory authority on trusts, where requested, to carry out an assessment of the needs of the carer of a disabled child, and it imposes the duty to take that assessment into consideration in deciding what services to provide. Article 19 also provides for support for children in need within early years provision. The implication, therefore, is that there will be provision for support for children with disabilities within early years provision.
226. The Children (1995 Order) (Amendment) (Children's Services Planning) Order (Northern Ireland) 1998 also placed responsibility on a range of agencies to plan together in relation to children's services. The four legacy children and young people's committees, which are the operational arm of children's services planning, are now being condensed into one regional strategic partnership for Northern Ireland, which will have its first meeting in January 2011 after the RPA arrangements.
227. All the key strategic drivers of OFMDFM's 10-year children's strategy Our Children, Our Pledge and the departmental family support strategy Families Matter draw heavily on the UN Convention on the Rights of the Child and the UN Convention on the Rights of Persons with Disabilities, which do not determine criteria, other than need. Those conventions have been ratified by the UK Government and, in the case of the UN Convention on the Rights of Persons with Disabilities, also by the European Commission.
228. The strategic and legislative principles within children's services are based on the requirements to consider a needs-based and person-focused assessment, and they should not be determined by criteria such as diagnosis, but on the basis of child/adult/carer first. I will quickly refer to the Carers and Direct Payments (Northern Ireland) Act 2002, which commenced in 2003. That legislation also provides a statutory right to a carer's assessment and makes similar provision for adult services as is provided for children under the Children Order.
229. Various work has been taken forward by the Department, which established the regional implementation team to look at providing consistency in models of service provision in children's services. That work resulted in the introduction of the understanding the needs of children (UNOCINI) assessment framework, which is a model for all children's services and is applicable to all agencies. Significant investment in and the roll-out of training for UNOCINI have been progressed, and a similar piece of work is now been taken forward on developing a tool for adult assessments. The legislative duties under the Chronically Sick and Disabled Persons Act are trans-generational and have relevance to children and adults.
230. In going through the various legislation, we want to point out that a wide range of statutory provisions is in place and seeks to provide a range of supports and protection in law for those with disabilities, including those with ASD. The determination of need, which is focused on the assessment of an individual's unique circumstances and needs, in conjunction with that individual carer, is the primary focus of service delivery.
231. The Bill references the need for robust data collection and the utilisation of such data in planning. The board has a number of data collection processes in place, such as the child health information system, which allow for the collation of prevalence of conditions by diagnosis, age and locality.
232. Work is also under way to complete a children's services plan and database that can provide not only a breakdown of disability by local government area, but a directory of services available in those localities.
233. The Chairperson: Mrs McAndrew, we are a bit tight for time. Many groups are due to give evidence, and we are trying to be fair to everybody by tying the presentations to 10 minutes. We have your document in front of us, so, when answering questions, feel free to deal with the points that you may not have made. For witnesses generally, it is better to start with a critique of our support for the Bill and then go on to more general points.
234. Mrs McAndrew: I apologise if we have done it the wrong way round.
235. The Chairperson: You are the first group, so I want to lay down some rules for the other groups.
236. Ms S Ramsey: Thanks for your presentation and your paper. I take on board the point about the Children Order, which you described as the primary legislation on the issue et cetera. However, the Order's provisions do not always get through to some of the parents with whom I have dealings. We need to live in the real world and accept that that does not always happen. Sometimes, the law says that individuals are supposed to get A, B, C, D and E, but instead they receive the most basic package of help, if any. Recent court cases and judgements have shown that to be the case.
237. It is probably not fair to put my question to you; I should be putting it to the Minister. The Minister is keen to talk about parity legislation, parity with England, parity with here and parity with there. Why are we not seeking parity with England on this issue and trying to find instances of best practice there?
238. Secondly, I take on board that much good work has been done by individuals, groups, organisations and parents. However, you talked about the groups that meet at a senior director level across the board in the sectors of health, education, employment, criminal justice, et cetera. Are they working?
239. You went on to talk about the non-governmental organisations (NGOs). I do not see that parents feel the impact of some of the work that is done at that level. If we are trying to strengthen your hand, as officials, to ensure that you have a statutory duty, the relevant legislation must exist so that you have the necessary resources to kick-start that statutory duty. The Children Order is a statutory duty, but, in some instances, does not have an impact. We can quote recent court judgements to support that, such as the one in Fermanagh a couple of weeks ago.
240. Mrs McAndrew: I will reply first, and Stephen Bergin will respond to the question of NGO involvement in the RASDN.
241. In our presentation, we were coming to the point that a range of extant legislation can make supports and assessments available to the full range of children and adults with disabilities. In fact, the judgement in the Fermanagh case that you mentioned underpinned that and said that the legislation provided for that to happen.
242. Ms S Ramsey: The support was not followed through.
243. Mrs McAndrew: The challenge within that is continuing to meet the demands and the needs of the people who need our services as a consequence of the provisions in the legislation. That case demonstrated the challenge that exists, in a full range of services, of continuing to meet that demand. If the conversation is about whether legislation is required to make that happen, the provisions exist in legislation already. The challenges are not with the legislation but are somewhat separate to that. They are about meeting demand. Stephen may wish to talk about NGO involvement.
244. Dr Stephen Bergin (Regional Autistic Spectrum Disorder Network): It is important to recognise that the work that I have been leading is relatively recent. It has taken quite a while to assemble the project structure. The action plan arrived in the summer of 2009, but we have been talking about autism for the past two decades. It took between six and nine months to assemble the full project structure, and a key part of that was to get our parents, carers, service users and voluntary agencies on board. The full project structure has been in place only since March 2010, and, eight months later, we still are in our infancy.
245. Even in those eight months of having the full project assembled, we have made significant progress. When I was first here as part of the independent review, the big issue was waiting lists. Those were measured in years, which was totally unacceptable. That is no longer an issue, in general. across Northern Ireland. By April of next year, we will be on target to meet the existing 13-week elective care target in priorities for action. Four of the five trusts are on target, or thereabouts, and the Belfast Trust is the last remaining one to get on target.
246. During the initial months, we spent significant time standardising the previous dozen or so diagnostic care pathways across Northern Ireland, which reflected the 17 former trusts, into a uniform single diagnostic care pathway. That will be launched in the next few weeks, and it has taken a great deal of effort from the professionals. A key part of that has been the input of the parents, carers and service users, in that they are, effectively, co-authors of that important document, which will come out in the new year. The parents, carers and service users have done significant work to draft those documents, and a great deal of work is going on in the background.
247. The investment that we put in from the Department, which is now £1·64 million recurrently, is all going into front-line services and front-line practitioners, who will have a cohort of lead ASD co-ordinators across Northern Ireland — one in each trust — and have oversight of a dedicated and specific team for ASD in each trust area. Some of the investment is still going into the services, and, by the time that all of it hits the ground, there will be a service in, for example, the Southern Trust with 17 or 18 practitioners, that was not there in previous years. Those practitioners are being recruited now, some of them in the current financial year. If you invite me back here later in 2011, those practitioners will be bedded in. and you will see significant services in the trusts.
248. The Chairperson: I remind members that we are discussing the DDA, not the strategy. The questions should be on the DDA.
249. Mrs O'Neill: My question is on the DDA. You are very welcome to the Committee, and I am aware of the work that the network has done. I put on record that I commend that work, particularly that of the parents, carers and service users who have been involved. You said that the DDA is all-encompassing and does not need to be amended. Why does it not need to be amended, and why would amending it cause a problem?
250. Mrs McAndrew: The DDA is viewed as all-encompassing because it is specific to disability, and children and adults with autism are viewed as being children and adults with a disability. Our one concern about amending legislation to make it more autism-specific is that it would mean focusing on one type of disability, and there is no specific legislation for each disability. The DDA was intended to be a generic, all-encompassing piece of legislation.
251. Your researchers referred to supplementary guidance that has been developed in England, Scotland and Wales, which may be a more appropriate route through which to make that explicit and clear, but, from the practitioners' perspective in health and social care, we view the DDA as all-encompassing.
252. Mrs O'Neill: The legislation, as drafted, suggests an amendment to insert the words "social and communication". That amendment extends beyond autism.
253. Mrs McAndrew: That is correct.
254. Mr McShane: The issue with the term "social and communication", and the debate has touched on some of the points, is that the Department recently issued another consultation on a speech and language action plan, which recognises the broad needs of children with speech and language and communication difficulties. A significant proportion of those children will receive a service: speech and language, early intervention or dealing with early identified developmental delay. Following that intervention, a significant proportion of those children will have most of those particular issues addressed. The concern is that a significant number of children have speech and language difficulties at present. We know that our services will intervene and that there will be good prognoses for those children, but should they all be covered in the DDA under disability?
255. Mrs O'Neill: I hear what you are saying, but why not? That is the first thing that came into my head. If the Disability Discrimination Act were amended to include "social and communication", it would reach out and protect those kids who have speech and language developmental problems, so why not?
256. Mr McShane: The point was made that, for some of those children, the duration of some of those difficulties could be quite short-lived over their lifespan. It could be one or two years. Once they start school, they receive the additional benefits of the education system, such as socialisation and speech and language therapy input. That changes the children, and they make significant progress in that period. It is not a lifelong disability per se. We know of a number of children who have developmental delays for a number of reasons, some of which will be diagnosed and some of which will not, but we have services in place to address those. We deal with them through generic and core services, such as speech and language or occupational therapy, and the same issues apply across a range of disabilities.
257. Mrs McAndrew: Our view of the DDA is that it affords protection to a group of people. It recognises that people with a disability have certain rights. It does not provide access to services. As I said previously, that is by way of an individualised need assessment of need. Our approach to assessing and supporting need, notwithstanding the challenges of demand, is that we regard disability as all-encompassing.
258. Mrs O'Neill: You made the point that the DDA affords protection to all children, but it does not. One of the cases that was raised with the Committee a number of weeks ago involved someone who had applied for disability living allowance (DLA) but was refused, because autism was not included in the Disability Discrimination Act. We had the papers to show that that was the reasoning from the tribunal. Surely widening the scope of the DDA to include "social and communication" would work in that person's favour?
259. Mr McShane: I will replace my professional hat with my parental hat. When I was before the Committee previously, I shared the fact that I have four children, three of whom have separate disabilities. From my considerable experience of working with families, one of the major issues for Down's syndrome families is the fact that they do not receive DLA other than through an appeal, because the structure of the form precludes some elements of the condition. The issue about changing the DDA to include autism is that, in some respects, some of the DLA forms are better suited to ASD than to other conditions. That is well known and well evidenced by Down's syndrome.
260. Mrs O'Neill: Thank you for that. It is important for us to look at the whole picture and try to get our heads around it.
261. The Chairperson: You made a strong statement in your submission that you did not get a chance to come to, Dr McAndrew. It states:
"The HSCB would contest this assertion and would be concerned that legislation pertaining to one disability will create the potential for a hierarchy of disabilities and will create greater inequalities. At this point in time there is no legislative provision which relates to any one condition such as Down's Syndrome, Cerebral Palsy etc and to create such distinctions is at variance with good practice".
262. That point has been made before. Those on the other side of the argument say that, when other legislators have defined autism as a disability, there has not been a stampede of other groups who represent particular conditions demanding parity of legislation. People whose relatives have Down's syndrome, cerebral palsy and other complex conditions do not demand that they be brought within the definition of the DDA. What makes you believe that the Bill is the thin end of the wedge and that it would cause problems in the future?
263. Mrs McAndrew: Our perception is that the Children Order and the DDA are all-encompassing. It is of concern to us that the focus would be on specific conditions rather than on the broad spectrum of people with a disability. We should look across our services — universal services as well as specialist services — to support people with disabilities who live in our communities.
264. We contest the notion that not including autism in the DDA creates inequalities. We are expressing, for the Committee's consideration, our view that the perspective should be one of creating more integration and universality, rather than of defining people by their medical condition. We seek to approach people by assessing their whole-life situation rather than relying purely on a medical diagnosis to access certain services. I come back to the fact that we are talking about individualised and person-centred assessments, rather than diagnoses being the lead elements.
265. The Chairperson: Along with Mickey Brady, I have spent many hours attending tribunals in Ballybot House. In the real world, when a person goes before a tribunal, hard legal hooks are sought on which to hang the award of DLA, carer's allowance or whatever. If autism or a related condition does not appear in the legislation, the outcome is that the appropriate benefit cannot be awarded.
266. I am still slightly intrigued as to why making the DDA more embracing and comprehensive would lead to inequalities. I would have thought that making certain that everyone who has a disability is included in the DDA would place everybody on an equal footing. Someone who has a broken leg, for instance, definitely scores points, as does someone who clearly has acute depression, but someone who has autism does not tick either box. I am missing something, and I would like you to expand on your thinking.
267. Mrs McAndrew: We take your point.
268. Mr McShane: I cannot comment about other Departments, agencies or services concerned in health and social care. Reference was made to the International Classification of Diseases (ICD) 10 definition that autism is a disability. I note the comments that were made about the Welsh model. If you examine that in the context of the Northern Ireland family support model contained in Families Matter, it clearly has a tier 1 to tier 4 structure as well. That gives access to all at a universal level, and, moving through the tiers, to a specialist intervention. We already have a Province-wide departmental strategy, which has been rolled out and encompasses the particular issues about that eclectic approach.
269. I am a commissioner for children with disabilities. Many of the issues related to autism are also identified by families with Down's syndrome, cerebral palsy, and so forth. Those issues include access to special needs assessments in schools, access to respite and access to transitions. There is a commonality in the world of disability, and, sometimes, that provides strength in trying to address the issues. Such commonality has an overall benefit.
270. Mr Easton: Thank you. Fionnuala, a wee minute ago, you used the word "perception", which concerned me. You described it as your perception that "social and communication" should not be included in the DDA. Perhaps I am not the only one who picked up on that. What you tell us is, therefore, not a reality: it is just your perception. Do you see what I am saying? I want to point out that other conditions, such as fibromyalgia, are not supported under the DDA. It is a medical condition. Therefore, other conditions that are not covered by the DDA must also be considered. It worries me that you have not come to us with hard facts, but with perceptions.
271. Mrs McAndrew: We expressed our view from the Health and Social Care Board's perspective. It is difficult for us to comment on another Department or another agency's practice and procedures. I am not quite sure what facts I could present to you. We are concerned about moving away from a generic piece of legislation, which should pertain to all people with disabilities, and becoming quite specific about those who are included or cited in the legislation and those who are not. We are drawing that to your attention this afternoon.
272. Mr Easton: Please, excuse the way that I phrased my comments. Kieran, you mentioned that the autistic spectrum is broad and that, perhaps, it should not be included the DDA because — if I frame this in the correct terms — the condition might last for a couple of years or could, sometimes, be lifelong.
273. Mr McShane: No. I want to clarify that. I made the point that some speech and language difficulties can be short term, whereas autism is a lifelong condition. We get feedback from our colleagues in the Department of Education and, certainly, from speech and language therapists. Part of the rationale for the recent action plan was to help to address some of those broader generic speech and language and communication issues that are being identified and will, now, be challenged through that particular action plan for speech and language.
274. Mr Easton: Thank you for clearing that up.
275. Mr Girvan: Thank you for your presentation and submission. You have demonstrated with your evidence that the DDA does not cover every condition. You said that there are a number of failings in your systems, in diagnosis and in ensuring that people are seen and dealt with fairly, and that it is only since the strategy was introduced that you have attempted to catch up and put something in place to ensure that people are seen within a reasonable time. If people were to present with major depression, they would be treated immediately and would not have to wait some time for their problem to be diagnosed. That is part of the issue. By saying that the DDA covers everything, you give yourselves a get-out clause. You are not addressing the issue correctly. It is necessary that ASD be included. You mentioned that you deal only with your own agency. The Bill in its entirety will deal with other agencies, which require some form of cover to ensure that they deal with issues through legislation. We must ensure that that point is covered. Will you explain whether the strategy was the only thing that kicked you into operation? The condition has existed for ever, yet it is only relatively recently that matters have started to fall into place. I appreciate that the Department has, probably, had to react to the issue in light of the Bill's being proposed.
276. Mrs McAndrew: I will ask Stephen to comment on that.
277. Dr Bergin: The Health and Social Care Board has existed for only the past 18 months. Prior to that, I was with the Southern Health and Social Services Board, where we had a strategy in place for a decade. The Department provided investment for children's services; Kieran has been highly involved in that. Other board areas had their respective strategies, although, admittedly, not all of them. We have gone from a situation in which there were 17 or so trusts down to five. The scenario and the lay of the land are, therefore, quite different. However, we are not at a baseline of zero. It is not as though we only started during the past 12 or 18 months.
278. Mr Girvan: I appreciate that.
279. Dr Bergin: The action plan has just started.
280. Mr Girvan: However, it has taken a long time for that to come into operation.
281. Mrs McAndrew: In addition, we have been dealing with increasing demand for years because of the rising number of people being diagnosed as autistic. There has been an issue with waiting times for access to assessment and treatment, but I am not sure that that means that we have not recognised autism as a condition under the DDA or that we have not been trying to deal with it. That has posed us challenges in respect of the length of time that people have waited for assessment and treatment. However, through investment over recent years and by particularly focusing on that area, we have made significant improvements.
282. Mr Girvan: You said that an increasing number of people are being diagnosed.
283. Mrs McAndrew: Statistically, that is the case.
284. Mr Girvan: Are you saying that the sector is ever increasing, or have those people always been there but never been diagnosed? Were they, therefore, being failed by the system?
285. Dr Bergin: It is a mixture of new cases in the younger age groups and an older, prevalent cohort that has been there for years and is, perhaps, now being detected. The age of diagnosis has decreased in recent years. Ten years ago, diagnosis was at an average age of five or six but it is now much earlier, at about two or three years of age.
286. I will pick up on a point made earlier, which is that an autism diagnosis cannot be rushed. We are talking about somebody presenting within a maximum number of weeks, but the diagnosis process is complex, as members probably know, and we are putting in place a standardised, agreed process by which to address that. It is rare for someone to come through the door and leave with a diagnosis of autism after one session. Rather, diagnosis is an iterative process over months of observations.
287. Mr Girvan: I appreciate that, but I come back to the perception that the Disability Discrimination Act 1995 encompasses everything. Relatively recently, I dealt with a mature lady who had problems, and she was in her 40s when she was diagnosed as having an autistic spectrum disorder. That lady had been failed by the system. She had been treated for all manner of social problems without her condition ever being properly diagnosed. It took some time for that to happen, and then it was only through referral and the proper process. However, until recently she was failed, so we are not even talking about the situation 10 years ago, because that happened in the past 18 months. That lady was 40 years of age. I appreciate that the condition is being picked up in people earlier, but that lady had lived her life thinking that there was something seriously wrong with her, and she was relieved to find out that she had a condition for which she was able to get help.
288. Dr Bergin: Much of the emphasis has been on children, and we need to catch up with adolescents, younger adults and older adults. I have told the Department that that must be a bigger thrust in the strategy. We are working on the adult diagnostic care pathway now, and it will follow hard on the heels of the children's care pathway. We hope that, by around the start of the next financial year, each trust will have a diagnostic hub for adult services. That is looking forward, but I agree that there are deficiencies in adult services.
289. The Chairperson: Members, we would like to be home for Christmas. We have not yet finished the first round of questions on the DDA, so Pól Callaghan will be the last to ask a question on that subject before we move rapidly on to the strategy issue, unless anyone has a burning issue that has not been raised.
290. Mr Callaghan: Chairman, you will be pleased to hear that I will be brief. The last paragraph of the briefing — members received the table only today, so we are working on the hoof — states:
"There is a danger that when citing disability as determined by condition alone, that this lends itself to an interpretation of a medical model which is reliant only on diagnosis"
291. Is it not the case that the DDA part of the Bill does not rely on diagnosis at all? The Department told the Committee that the provisions did not rely on diagnosis. It seemed to think that that raised issues about autism not being specified in the DDA-related part of the Bill. I am just not sure how that paragraph of the submission relates to the DDA provisions in the Bill.
292. Mrs McAndrew: The final sentence was more general; it was not specific to DDA. However, generally speaking, and for our purposes, the existing legislative provision includes autism. We are a bit concerned that the Bill would create a model, across health and social care provision for people with a disability, that would be based on the social model of disability. Our concern is about too much focus on the stipulation of autism in legislation. I do not mean that it would be a step backwards, but it would create a new perception that a medical diagnosis would be required to access services and support. The Health and Social Care Board has tried to move that situation forward so that a medical diagnosis is not the only way to access assessment and support.
293. Dr Bergin: The definition of someone's needs within the term "autistic spectrum disorder" does not convey sufficient information. All sorts of co-morbidities come with individuals. The co-morbidity may relate to mental health, epilepsy, gastric conditions, and so forth; the list goes on and on. The term "autism" could have a wide spectrum of meanings, because it is divergent in its individual presentations. The point of that sentence is that the presenting need should be assessed.
294. Mr Callaghan: We are not talking about the DDA clause, because it does not include the word "autism" — indeed, some people have an issue with that. Therefore, we are talking about the provisions in clause 2 and beyond. However, the Department is already rolling out an autism strategy. Given that the Department's entire argument to the Committee, and, it is fair to say, the board's argument today, strongly rely on the fact that services are already being rolled out, I do not understand any principled objection to the specification of autism in clauses 2 and beyond. That objection formed part of Dr Bergin's presentation in particular. That is entirely commendable, but I do not understand why that is an issue as far as the Bill's provisions are concerned. Do you understand what I mean?
295. Mrs McAndrew: I understand your point. Our view is that, when it comes to enacting the Bill, the extant legislation is an enabler. The judgements that we have had and the cases with which we have dealt make it clear that the extant legislation is an enabler of the provision of services and supports to people with autism. That is the crux of our presentation.
296. The Chairperson: Is your question on the strategy, Kieran?
297. Dr Deeny: I have a quick question on the DDA.
298. The Chairperson: As long as it is quick: in case I ever get knocked down near Omagh, I have to be careful.
299. Dr Deeny: I take on board exactly what the three folk said, and I agree with much of it. I thank them for coming today. Is the point that people are uncomfortable that the one named disability will be autism, whereas we are dealing with many different disabilities? Cerebral palsy, Down's syndrome, muscular dystrophy and all sorts of genetic disorders have been mentioned. Is the concern about a hierarchy of disabilities?
300. I agree with Stephen that many people with autism have significant additional problems. The whole person must be taken into consideration. As a medical professional, I agree that the Bill should not be in any way construed or constructed so that decisions are made based on medical conditions. The focus must be on need, and a holistic approach is required.
301. Mr McShane: I will speak from a personal perspective. My wife and I have four children: one has autism, one has Down's syndrome, and one has undiagnosed speech, language and developmental difficulties. Our fourth child is a little girl, and I am extremely concerned about her. She does not have a condition, but I worry about the impact on her needs. In the world of autism, it is not uncommon to have more than one condition in the family. Is it right that, within one family, the premise should be based on the fact that legislation exists for one child, as opposed to a process that focuses on the individual needs of all children?
302. I argue that the child who has the greatest need is probably the one without the condition, because of the impact of the others' conditions. At present, our legislation, strategy and practice ensure that we have a holistic assessment of a child and a family in the context of our family support model. From a personal perspective, that leaves me much more satisfied that we are dealing with the issues within the DDA. In some ways, legislation will not change things. The important thing is the application of services on the ground and the impact —
303. Mrs McAndrew: In case there is any doubt, we understand that the proposal for the amendment to the DDA does not specify autism. We are not trying to ignore the fact that it talks about social and communication issues.
304. The point that we are trying to make is that the provisions of the current legislation extend adequately, in our view, within health and social care, to people with autism.
305. The Chairperson: We must now move on to the strategy.
306. Mr Easton: It appears to me that the Department's strategy has no impact on or relationship with other Departments. That is why it is not working to my satisfaction. I cannot speak for anyone else. The Bill forces all Departments to co-operate, organise training, and so forth to address autism and the issues surrounding it. Do you not believe that that is a much better approach than the one that the strategy offers?
307. Dr Bergin: One would think that I was expected to sort out the world of autism for Northern Ireland. How long would that take? It was never going to happen in one year. We must be realistic. It takes time to build up relationships with other agencies and with the personalities involved. I have been working on that. The key focus was to build up that relationship with education. In every trust and in every regional group, there is a key relationship with educational psychology and education sector staff. They provide advice to those groups.
308. That has worked the other way as well. Kieran and I are members of the education sector review team of the autism review. A key link has been established with the education sector, and we intend to progress that in the new year through more joined-up thinking, from the top down in the Department, between health and social care and education to create a more structured, robust way forward.
309. With regard to other agencies and sectors, relationships have been built up, and I talked about those regionally and locally in trust settings. If members were to go to the Southern Trust, they would see the relationships with the various agencies, for example, Craigavon Borough Council, where partnerships have been developed on leisure services. The relationships are being built up bit by bit across the region but, as the Committee will appreciate, the building of so many relationships with so many agencies is a highly complex process, and it takes time.
310. Mrs McAndrew: The board believes that integrated planning across agencies and Departments is critical to meeting the wide-ranging need of anyone with a disability, including people with autism, as a principle. An example of that is through children's services planning, which is a mechanism that we employ. Currently, there is no statutory duty to co-operate under children's services planning, but we have an effective, multi-agency planning system that has been running for nearly 12 years. In principle, it should be integrated, multi-agency and multi-disciplinary.
311. Mr Easton: The Bill, therefore, is a good development.
312. Mrs McAndrew: In principle, it can be achieved, and it is achieved elsewhere in our planning and commissioning of services.
313. Mr Easton: However, the Bill would force you to do it, right across all Departments, whereas now you sort of do it, if you know what I mean. Do you not feel that having all Departments involved could lead eventually to extra moneys coming in from other Departments for autism? Equally, their training would help to get people with autism diagnosed more quickly and help them to meet their specialist needs. That applies not only to education and health but to the Department for Social Development (DSD) when it comes to possible benefits and to the Department for Employment and Learning (DEL) because people at university also have autism. Do you not think that savings could be made there?
314. Mrs McAndrew: As far as being forced to work on a multi-agency basis, that is a principle to which we already adhere. We have a range of examples where we do that without the force of legislation, because it is the right thing to do. It is good practice, and it means that we can give consideration to how we pool our resources, whether money or staff on the ground, to support a range of people. There are many examples of how that is achieved without our being forced by legislation.
315. As for working with other agencies, education is a particular example of funding being set aside over recent years for autism services. Within the trusts, there has been an engagement with education to consider how their money and our money, together, can develop more effective resources in a locality, rather than Departments simply thinking about their own money. Those pieces of work are ongoing.
316. Mr Easton: Do you not feel that the training that the Bill would enforce on all Departments would be beneficial to you? That does not happen at the moment.
317. Dr Bergin: You would be surprised at the amount of training that is going on. We have just completed a baseline scoping. This is part of the problem with training initiatives in Northern Ireland: it is a joint venture between us and the education sector, and we found 277 different initiatives across Northern Ireland, which is a small area. That needs to be co-ordinated, tied down, prioritised, structured and managed, but that is not happening. Our plan is to make it happen and to get it structured and prioritised. It would be wrong to say that there is no training across agencies; there is.
318. Mr Easton: Does the Department of Agriculture and Rural Development (DARD) carry out training?
319. Dr Bergin: I would have to go through the list of the 277 initiatives —
320. Mr Easton: I am talking about Departments.
321. Dr Bergin: I cannot speak for DARD, but I can tell you that there is an extremely long list of initiatives. It surprised all of us how much training is going on. It is primarily baseline awareness-raising training, as opposed to professional-type initiatives.
322. Mr Easton: Do you know whether the Department for Regional Development (DRD) or the Department of the Environment (DOE) provide training?
323. Mrs McAndrew: We can provide the Committee with a report on the training initiatives and who is involved, if you would find that helpful.
324. Mr Callaghan: I want to start with the point on hierarchy, which you raised in your briefing paper. The Chairperson also mentioned it. Are there specific strategies within the board for Down's syndrome and cerebral palsy? Is it not the case the Department has itself recognised that autism is different, in that it has a dedicated autism strategy?
325. Mr McShane: The ASD action plan was issued at the same time as the acquired brain injury action plan. One of the issues with strategies and recognising that there are issues for ASD was the acknowledgement that other conditions also have issues. Currently, approximately 6,000 children each year acquire minor brain injuries. There is no legislation for them, but there has to be a strategy on how they are followed up and what happens in relation to best practice and providing the best service for those children, many of whom manifest the same attributes as a child who may present with ASD. We have several strategies for issues that are pertinent to particular groups. I cited the example of acquired brain injury, the strategy for which was issued at exactly the same time as the ASD strategy.
326. Dr Bergin: Wearing some of my other hats within health and social care, I head up work across eating disorders, addiction services, forensic mental health and people with personality disorders. The Department has issued a whole raft of network and strategy areas. It is not unusual to have action plans across all sorts of discrete areas.
327. Mr Callaghan: It is not a criticism of the fact that there is an autism strategy, far from it. The Committee will have to consider the impact of the argument, because it seems that nothing is required in the Bill to which the Department or the board has a principled objection. You do not seem to be arguing against any one action that the Bill requires of the board. In many instances, the board's argument is that it is doing certain things anyway. The issue seems to be with the statutory requirement.
328. Your briefing mentions dual diagnosis. There is nothing in the clause amending the DDA that prevents the application of the DDA to anyone with a dual diagnosis. The clause does not mention duality of diagnosis, but autism is the threshold at which the DDA applies. It not an exclusivity clause that excludes people if they have autism and some other condition, including some of the examples that Dr Bergin provided.
329. I assume that the current strategy provides for people who have dual diagnoses or multiple diagnoses, and I do not understand why a strategy as mandated by a statutory duty in the Bill would not be similarly facilitating of people with dual or multiple diagnoses.
330. Mr McShane: There is a level of complexity to the response, so bear with me. We have a number of children who are now diagnosed as having a disability, and very few childhood disabilities come on their own. Unfortunately, there tend to be associated conditions with them. For example, some of the major issues with Down's syndrome are sensory difficulties in the form of, for example, hearing loss and so on. There are a range of issues.
331. Coming back to the point that was made earlier, our focus is on the assessment of need in regard to the individual child and their family. That need is not premised on the fact that a child has a range of conditions or on the impact of the autism per se, but on the impact of the condition on the child and the family and how that changes the child's and family's life. A point was made on the recent judicial review. That review cited clearly that the failure in that instance was the failure to look at the wider context of the whole family.
332. On your question about dual diagnosis, we have x number of children coming through our system with complex medical needs who would not have survived ten, or even 5, years ago. A lot of those conditions are not recorded on any list for the DDA, yet those children still have very complex needs. It is an ever-evolving problem, and we have ranges of complexity in children's disability services, and that is pertinent not only to autism. If you were to ask me what is more important for a child whose co-morbidity is autism and Down's syndrome, my response would be that the needs and circumstances of the child should be assessed.
333. The Chairperson: Mr Callaghan, do you have another question?
334. Mr Callaghan: I have one more.
335. The Chairperson: I will come in on that and steal your valid point. I apologise profusely to the Deputy Chairperson for stealing her slot. Pól made the interesting point that a cross-departmental strategy might bring synergies and efficiencies that will save money. That was the first time that I heard that point being made, and it strikes me as an extremely useful suggestion. Has the Department or the board considered that as an option to reduce their opposition to the idea of preparing a strategy?
336. Mrs McAndrew: Do you mean a specific autism strategy?
337. The Chairperson: Yes, it is logical that, if all Departments were to co-operate on a single strategy, waste and duplication would be bound to reduce.
338. Mrs McAndrew: On a general basis, that is correct. I cannot quantify what the efficiencies and savings might be, but, previously, I referenced children's services planning, and that is exactly the principle behind that. We are looking at strategies that mean that all agencies that have something to offer to an individual or a family work together in considering how they provide the services. Very often in the past, that work took place in silos. To develop a more comprehensive service across all of the agencies, we must examine how we can develop a plan that means that we all consider the part that we contribute to the family or the individual.
339. As a principle, that is beneficial to the families and the individuals, and it helps to contribute to more productive and better quality services and more efficiencies. We are considering that model in a range of areas.
340. The Chairperson: Are you not making his point for him?
341. Mrs McAndrew: I agree with the point about multi-agency planning and delivery of services.
342. Dr Bergin: There are deficits, particularly in certain services, that another agency could not duplicate. We have to work in partnership with other agencies, but if I am looking for structured psychological therapies within adult services, other agencies will not be able to contribute to that. They will assist with an individual's wider needs, whether that is housing or leisure, but additional services are required.
343. As I said, we have done a great deal of work on the children's side, but if our next focus is to be on adult services, unless more money is contributed to health so that we can acquire the necessary practitioners and therapists, we will require a significant amount of new resources.
344. Mr Callaghan: Given the time frame, it would be helpful if you could give the Committee some idea of what potential additional resources might be required.
345. I do not mean to put people on the spot, but Mrs McAndrew, you talked about more integration and more universality. However, it is not unfair to say that the Hansard report will show you that we were talking about that happening within the realm of the board's competence.
346. Dr McShane said —
347. Mr McShane: It is "Mr". I am a social worker.
348. Mr Callaghan: It would be easier if I were to call you Kieran, because you can call me Pól. The same goes for everyone else.
349. I cannot comment about other agencies and other services. However, when the officials from the Department were here, they told us that they did not have a clue about what was in the DENI strategy. They explained that that was because DENI had not published its strategy, which was only at the developmental stage. I will not speak for the whole Committee, but when my party colleagues and I hear things like that, we become seriously concerned about the lack of co-ordination.
350. Fionnuala, I understand what you are saying about the aspiration to co-operate and what you and Stephen were saying about the co-operation that has been going on. We are trying to help you to better achieve your goals by forcing Departments and agencies outside your remit to co-operate with you and deliver services in a better way.
351. To be honest, I am quite puzzled by the pretext of the board and the Department, which is one of hostility to a Bill that, as far as I can see, is all about helping to deliver services and, in many ways, getting other agencies and Departments to provide assistance to you.
352. Mrs McAndrew: We welcome any measures that help us to work more collectively with other agencies. The concern is that we have examples of how we already do that without being forced to do it through a legislative requirement. We do not need a Bill to tell us to work with people and to co-operate with them.
353. The board will welcome any guidance or strategy that comes forward and helps us in our endeavours to make that a reality, so that we can work more effectively together to deliver more effective services for people. However, having considered the clauses in the Bill, we are not convinced that we need legislation to achieve that.
354. The Chairperson: I apologise to the Deputy Chairperson. I got a bit confused because she gave way to let Alex in. I thanked for her that by leaving her out entirely. I will have to go at some stage during this session, and the Deputy Chairperson will take over. If she cannot stay to the end, we have to agree, as normal, on who will then take the Chair. That honour and appropriate remuneration normally falls to Alex, but that is just tradition and custom, it is not a rule. If members are happy enough, Alex will take over if the Deputy Chairperson has to leave.
355. Mrs O 'Neill: With the best will in the world, other Departments will always be a wee bit reluctant to assist or to get involved while there is a lead Department. During the debate on the Safeguarding Board Bill, we discovered that having a statutory duty to co-operate is beneficial. I think that that would do no harm, in fact, it will help, and, as Fionnuala McAndrew said, the board would welcome any assistance.
356. One clause requires trusts to provide data on the prevalence of autism. In your submission, you stated that that was already being done. Among the issues that we have come across is that we cannot get statistics, figures or a breakdown in answer to questions about prevalence that are asked of the Department. Since it was established 10 months ago, I am sure that the network has had that experience. What are the biggest challenges that you face in trying to measure prevalence? What has the network done to address such problems?
357. Dr Bergin: All cases of people in younger age groups who present to primary care, educational psychologists and health visitors are now captured in the regional data system via a standardised approach. That data has been collected over the past 18 months or thereabouts. Therefore, children's services are recorded on a regional database, and those statistics are now available.
358. However, if we consider the adult population, the question is how many of those have presented to health and social care. It is unlikely that all of those individuals present to health and social care, and, therefore, only a proportion of them are in the system. Unless we undertake population-based studies at significant cost, how will we find those individuals, unless they present to health and social care or to another statutory agency? They are hidden. They have needs, but, unless they present to an agency with a diagnosis, it is difficult to ascertain how many there are. .
359. We can rely on fairly consistent worldwide and Europe-wide statistics that indicate how many people we would expect in each service across the full age spectrum. A population-based study in the adult field, at a cost of tens of thousands of pounds, may be the only way to do that. It has been done in other areas. What would it tell us that those international statistics have not already verified? It would tell us about individuals, but undertaking such a study would cost a significant amount.
360. Mrs O'Neill: However, it would be a study of benefit not just to those on the autistic spectrum, because you could —
361. Dr Bergin: I would not deny that.
362. Mrs O'Neill: Who asked the question of the Minister but could not get any statistics? That was brought up during the debate, but I cannot remember who asked the question.
363. Dr Bergin: Incidence statistics are much more reliable than prevalence statistics, the former representing the new cases as they come into the system, because we now capture those as they present.
364. Mrs McAndrew: That is only what is known to services.
365. Mrs O'Neill: That is obviously important for service planning.
366. Mrs McAndrew: Yes.
367. Mr McShane: On the issue that Mrs O'Neill raised, another strategy was recently launched that looks at sensory and physical disability. It has been difficult to try to break down those figures. That goes back to the issue of co-morbidity. If a child has, for example, three separate conditions, is he or she recorded three times? We have a broad child health information system database. There are currently codes on that system for: childhood autism, atypical autism, Tourette's syndrome, Asperger's syndrome and PDD, which are the conditions addressed in the Bill. That child health information system is under review by colleagues in the Public Health Agency, but it has been in place for the past 20 years. The issue has been one of its applications, but we hope that its existence will provide us with a template and foundation on which to build. It covers all childhood disabilities, not only ASD issues.
368. Mrs O'Neill: OK. Thank you.
369. Dr Deeny: It is good that we are discussing such an important topic. As I was going to the bathroom —
370. Mr Callaghan: Stop.
371. Dr Deeny: I should not be saying that, but we go to the bathroom from time to time. However, I thought that, with the carry-on in the city this week, we saw an awful example of how our disabled children are treated by others. We also saw the wonderful public response.
372. I remember you well, Kieran, not only because you have a good first name, but because you have three children. I hope that they are doing well. The strategy refers to the autism awareness campaign and the autism awareness training. I know that the campaign is simply a public exercise to make people more aware of autism. Perhaps you could summarise some of that.
373. Obviously, the training is more detailed for those of us who are involved, but it must include everybody. One of the briefing papers highlighted that teachers and health and social care professionals were not mentioned, but training will have to apply to everyone involved, not just those working with children, but those working with adults with similar conditions. What is the difference between the two, and what will it entail? Will the training be a large programme to roll out?
374. Dr Bergin: Our priority has to be the diagnostic care pathway, because that will be available to us now. Our priority is to implement that in 2011. We need to ensure that the expert, front-line, senior professional staff receive standardised, high-level, competent training in complicated areas of work. Our initial priority in 2011 will be to make sure that the cohort of staff in each of the five trust areas who are participating in children's diagnostic work — there are about half a dozen in each trust area — are all competent and fit for purpose to undertake a standard diagnostic care pathway.
375. The next bit of that work will be to implement the adult diagnostic care pathway. We will work with the Royal College of Psychiatrists and the division of clinical psychology to ensure that adult psychologists and psychiatrists are better able to undertake adult diagnosis. We had a workshop with them in June 2009, and they accepted that there is a lower level of expectation of adult services compared with children's services. Incrementally, over time, we will build up that expertise in diagnosis. Parallel to that, we will scope the need to undertake interventions in the training that practitioners require. If we had a wider range of resources, we would be proposing to undertake a much wider range of training, but we have to focus on the key priority areas in front of us now. Diagnosis and interventions are our focus in 2011.
376. Dr Deeny: As a GP, I suggest to the board that each trust is supposed to take a half day every quarter for learning for GPs. I know that the Western Trust stopped for a while, but it has restarted. Autism would be an ideal topic on which to update GPs.
377. Dr Bergin: I should have mentioned that all of our 600 or so health visitors undertook a half day or a full day of specific ASD training early in 2009. Across adult services in particular there is a wide range of social care staff, community psychiatric nurses, and psychology and psychiatry professionals. During 2011, I would like at least to ensure that, in your area, for example, in a community mental health team of six, eight or 10 people, at least one or two receive more advanced training. As you probably know, there is very little medical undergraduate, or even postgraduate, training in ASD, and we need to address that as a priority.
378. Mrs McAndrew: We will take that comment about GP training on board.
379. Dr Deeny: What is the difference between the two? Is the public training simply to make the public aware of people with autism or how to pick up on it quickly in, for example, shops?
380. Mr McShane: In our world, the focus is on those front-line staff who come into daily contact with children and families. As Stephen said, we have done some work with the health visitors, but social workers, care assistants, and so on are the face of the Health Service and have contact with the greatest proportion of the population. We need to make them aware of ASD issues and of its particular traits in order to tailor their support and intervention to the individual.
381. Dr Deeny: You are talking about the people who work with the kids — the professionals. I am talking about a broader base of the general public.
382. Mrs McAndrew: We are talking about the staff who work in universal services and the voluntary sector who may come into contact with those children. You are making the point about a much broader base.
383. Dr Deeny: Yes, because many people do not know what ASD or autism is. If you asked them about ASD they could not tell you what it is. It may be an opportunity to send out a message.
384. Mrs McAndrew: It is not something that the regional network has taken forward at this point, but we take that comment on board.
385. The Chairperson: That ends the second round of discussion, which was on the strategy. We will move on to any other items that members wish to raise in this session.
386. Mr Callaghan: I hoped that someone else would go first, Chair. Kieran raised an important issue about a hierarchy of disability. It is something of which we must be cognisant. As I understand the provisions of the Bill, and from reading what the Department said to us at their evidence session, it does not contain any specific financial provision. If there is no financial provision specified in the Bill, it seems to me that you cannot presume that any requirement will be put upon any public authority, including the board or trusts, to skew resources away from, for example, cerebral palsy services into autism services. The statutory duty on the health board, trusts or other agencies is essentially to set out how they will deal with autism through the strategy. I think that, with due respect, it is putting the cart before the horse to suggest that that is a reason not to enact the Bill. In a way, that goes back to the argument about not letting the perfect be the enemy of the good. Over a number of years or decades, future Assemblies may decide that there will be a Bill for cerebral palsy or for various other services. Who is to know? However, the issue before us is whether there should be a Bill dedicated to autism.
387. The Chairperson: Mark Durkan would be proud of some of your one-liners, Pól. You have been well trained.
388. Mr Callaghan: I promise that they are all mine, Chair.
389. The Chairperson: I must say that Pól has encapsulated what many in the Committee are thinking. You say that the system works well, but that you do not want it to work better. It is a philosophical argument that I also find difficult to grasp.
390. Mr McShane: As a country boy, I would probably retort with, if something is not broken, why fix it? We have clear diagnostic criteria that state that autism and associated conditions are disabilities. The same criteria apply across Down's syndrome and whatever. At this point, we are not making any distinctions across those particular internationally agreed criteria.
391. Mrs McAndrew: We think that we are working well and are doing everything that we can to implement the action plan. I respectfully suggest that there is nothing in our submission that indicates that we do not want to work better. We always want to work better. The only difference in our submission is that we suggest that the extant legislative provision directs our endeavours in relation to children and adults with autism. That legislative provision already exists. The challenges for us relate to demand and resources, not necessarily to the legislation. That is the crux of what we are saying. However, I say categorically that we will use every opportunity, all policy guidance and whatever might be the outcome of the Bill to work better. That is our intention.
392. The Chairperson: As there are no further points on the generalities, I thank you all very much. It has been quite a long session, and I am glad that members were able to elicit information on the sections of your submission that you did not reach.
16 December 2010
Members present for all or part of the proceedings:
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Mickey Brady
Mr Pól Callaghan
Dr Kieran Deeny
Mr Alex Easton
Mr Paul Girvan
Witnesses:
|
Mrs Arlene Cassidy |
Autism NI |
|
|
Mr David Heatley |
Parents' Autism Lobby |
393. The Deputy Chairperson (Mrs O'Neill): Arlene, Paula, Audrey and David, thank you for bearing with us for three hours until you could get to the table. I know that the issue is so dear to your hearts that you do not mind waiting. I am going to have to leave and Alex is going to take over.
(The Acting Chairperson [Mr Easton] in the Chair)
394. The Acting Chairperson: I welcome both groups here today. There will be a 10-minute presentation. Would one of your groups, or both, or all four of you, like to make a start?
395. Mrs Arlene Cassidy (Autism NI): I will start, and then —
396. Mr David Heatley (Parents' Autism Lobby): I will finish; if there is time.
397. Mrs Cassidy: An additional set of papers has been presented to the Committee. The first three pages have been tabled already. In the original papers, there is a point 9 — the additional papers expand the headings under point 9. The three pages presented originally are very much about context — the credentials of the charity, Autism NI, and our history. I do not intend to go through them now; I want to prioritise other issues that have not been submitted to the Committee; however, time may run out. At least members have the hard copy, and if there are any points of clarification, please feel free to contact us afterwards.
398. In addition, before I start, I noted the earlier discussion on the costs of autism. I want to submit a paper that Autism NI prepared as part of its early lobbying work. We can provide other copies. There has been a study carried out already, by Martin Knapp, regarding the cost of autism in the UK, including the hidden costs, the loss to the economy, the whole issue of misdiagnosis and the cost to parents and couples for caring where one person is not able to work and contribute to the economy and the family. So, an analysis is available; and there was one carried out in Australia and Canada. We briefly analysed that work, really just to register that work in that area has already been done which may usefully contribute to the Committee's discussion.
399. I will make a few key points, the first of which is on the present level of need. I am sure that members have the relevant information, so I will not insult them by going through it in detail. I could quote figures from recent research carried out by the voluntary sector, some of which were quoted in the Bill's Second Stage debate. I could quote prevalence rates from the Department of Education, which show that 5,000 school-age children have been diagnosed recently, compared to 900 in 2002. I could also quote targets set by the DHSS regarding waiting lists, the positives and the negatives. I could remind the Committee of the recent judicial review decision, referred to earlier, regarding autistic spectrum disorder (ASD) service failures. I could refer the Committee to the Autism NI report that catalogues the hours spent on ASD statutory service reviews and strategies. There is a companion document to that, which gives a history of work of health boards and trusts in the past, prior to the departmental action plan. I can encourage the Committee to consider the Assembly Research and Library Service's reports, and, again, members heard a further submission this morning. However, my final point on this is that the conclusion remains the same: there has been more talk than effective action. Prevalence rates have increased by 500%, but funding has risen by just 100%.
400. The next point that I wish to register concerns the human and financial costs referred to in the first two paragraphs of our submission. The cost of ineffective leadership and engagement on ASD in Northern Ireland is incalculable and shameful. By comparison, Wales is ASD-informed, systematic and professional. It has built on existing expertise and has not thrown the baby out with the bath water or reinvented the wheel, as Northern Ireland is doing under the cloak of service redesign. Families are reporting to us that the re-referral system — as referrals are recycled and targets are met — is one of the negatives in tackling the waiting list for diagnosis.
401. We will address the human cost by presenting a single case history. If the Committee wishes us to do so, we can elaborate on the detail when answering members' questions later. As regards the current system's capacity to meet needs, there is a family that is happy to share their information with the Committee. Their experience encapsulates the nature of the service breakdown and underlines some points that we will highlight. The family has a child whose school phobia led to a build up in volatile behaviour which culminated in the child presenting as a danger to himself and others. A GP and a consultant were involved in the case. The child locked himself in his room, and an ambulance and the police were called. Ambulance staff admitted a lack of awareness of autism and said:
"ASD complicates everything."
402. The child was admitted to hospital eventually. The doctor there phoned eight to 10 psychiatrists. That doctor's impression was that Asperger's syndrome complicates the matter, and said that they felt that the reluctance on the part of psychiatrists to come and see the lad had something to do with his condition. To get psychiatric support, the family had to agree to the 11-year-old boy being sectioned. The psychiatrist arrived 24 hours later. I have been given permission to read the parent's comments to the Committee. This is how the parent related her story on paper:
"Why did every psychiatrist on call refuse to treat my son? Why is there a bewildering confusion among professionals when it comes to dealing with a child on the spectrum? Why did my only support come from the autism charities? Why did I experience one single moment where I felt nobody would or could help me or my boy? This should not happen ever. A child with ASD should not be in any way discriminated against because of their condition, which is exactly what all those psychiatrists did. This should never happen again. It was, without a doubt, the most traumatic experience of my life, and of Finn's."
403. I want to address the issue of equality. I will not read through my briefing, because I know that time is not on my side. I met Brice Dickson and representatives of the Human Rights Commission this week and I have detailed their view of the Autism Bill in my briefing. They were profiling the work that OFMDFM will have to do to comply with the UN Convention on the Rights of Persons with a Disability, citing that as the rationale for not going forward with the Bill and waiting for that compliance to take place. However, as we know from history, there is no guarantee that autism will ever sit at the table, but we see the Bill as a guarantee that autism will sit at the table.
404. I will skip the rest of my briefing and move on to the impact on families. The Committee already possesses some of this information. I want to give a few examples that show why legislation is needed. Others who have given evidence today have referred to the fact that disability living allowance (DLA) guidance uses the current definition of disability in the Disability Discrimination Act 1995, which does not give clarity on autism. Physical markers dominate the DSD regulations on housing adaptations. The case study on the lack of awareness of autism by the ambulance crew showed that they lacked confidence in how to deal with the situation. The emotional impact of the legislation should not be overlooked. Recognition of autism has been a long time coming and the clarity that it brings to existing regulations should not be underestimated.
405. I want to make a few comments about the DHSSPS action plan and the Department of Education framework. I want to reinforce the comments made earlier that, no matter how effective something is or is not, things can always be made better. We believe that the legislation can only strengthen and empower that which is already happening. At the moment, there is limited buy-in from other Departments. The DHSSPS ASD strategy relies on a medical model, not a social model. The balance of resources has gone into diagnosis and not into early intervention or family support.
406. The Department of Education ASD framework does not include an operational partnership role for the voluntary sector. Significantly, the DHSSPS engagement model, with non-mandated carers and individuals with ASD, is reckless, because it is unsupported and unresourced. Leaving parents in that kind of consultation and implementation network unsupported and unresourced risks them ending up spent and burnt out. There is quite a demand. My point is that there was a submission for supporting those parents, but the DHSSPS chose not to accept it.
407. My final contextual point about the Bill is to do with its implementation. We are concerned about that; leadership is crucial and respect is essential. Later in our briefing, we recommend that there should be a link and partnership and some sort of agreement with what has happened in Wales, looking at examples of best practice across the devolved nations.
408. We have provided a written response to the Bill. Autism NI supports the changes to the Disability Discrimination Act 1995 in clause 1, mindful that correct criteria in the 1995 Act for key elements, such as those that deal with long-term conditions, will be in place as well as diagnostic evidence.
409. As regards clause 2, Autism NI supports the critical need for a cross-departmental strategy to establish lifelong services plans that ameliorate the particular challenges experienced by individuals with ASD across life transitions. That is really to say that we recognise that transitions are difficult, but there is a particular poignancy as it hits on one of the core impairments of the condition of autism.
410. Autism NI is mindful of the need to consult with, integrate and recognise the contribution of the voluntary sector and the families they represent and suggests that that be included as an amendment. If this request will delay the passage of the Bill, Autism NI will defer its request and address the point operationally. The overarching message that we would like to get across is that we would like to put forward amendments to the Committee in this paper, but the overarching and overriding consideration is that we do not want, in any shape or form, to cause any delay to the passage of this Bill, because there are other ways of tackling the issues afterwards.
411. As regards clause 2(2), Autism NI is mindful of the need for a time limit on any consultation between Departments as part of the Bill implementation process. There is no time limit specified in the Bill although there is a requirement to consult. Perhaps that is required. As regards clause 2(3), Autism NI wants to profile the fact that data collection is not just done by the Department of Health. Other Departments have been very effective in data gathering. We have been reliant on the Department of Education's figures for years. It is about sharing data and synchronising it across Departments.
412. On clause 3, Autism NI is mindful of the critical importance of quality, accredit-intensive, early intervention models such as those profiled by Autism NI through the Parents' Education as Autism Therapists (PEAT) programme, the Keyhole programme and other organisations such as PEAT and Centre for Early Autism Treatment (CEAT). We request the inclusion of recognition of the overwhelming evidence that supports the effectiveness of early years intervention. Once again, it has been suggested that an amendment would be likely to affect the passage of the Bill adversely, so Autism NI will address the issue operationally.
413. The point of early intensive intervention is critical in view of the previous point made that although diagnosis is an important issue resources have been allocated to the condition disproportionately. For parents who are wondering what they can do when they receive the diagnosis, the resources and the supports available are not in place.
414. In clause 3, Autism NI regrets the omission of the role of an autism advocate to secure progress, consistency, effective structure and much needed and respected leadership. Autism NI supports the need to explore that omission further, but is mindful of the issue of delay. Autism NI requests the consideration of a memorandum of understanding, particularly with the Welsh Assembly, to secure the required partnership assistance towards establishing effective implementation structures, especially in the oversight of joined-up and planned services across the transitions. What I am saying is that the Welsh strategy crosses three of our Departments. It includes health and social care, education and lifelong learning, so it goes right into adulthood.
415. Autism NI is proud to be associated with the Autism Bill and is hugely grateful to Dominic Bradley, the all party group members, and all the MLAs who have listened, studied and acted. Before I introduce David, I want, as chairperson of the carer's autism lobby, to record that the principal stand taken by this charity has remained constant to its political lobby dating back to 2001 and to its pledge in 2006 to campaign for ring-fenced funding, a cross-departmental strategy and legislative recognition for autism. I would like to register that with the Committee. However, since 2008, Autism NI has been subject to threatened investigations, withdrawal of DHSS regional board and health trust funding, as well as expulsion from the Northern Ireland Regional Autistic Spectrum Disorder Network (RASDN) reference group unless we gave up the aspiration to legislation.
416. In 2010, those threats were directed towards the new chief executive and the director of development. Yet, in comparison, in 2010, Autism NI won recognition of its principled, dignified and professional stand for social change from the voluntary sector, when it was presented with the CO3 Voyager Leadership award in political impact.
417. Autism NI may pay the ultimate price for its principled stand unless the position is reversed and relationships are actively reconstructed.
418. I would be grateful if the Committee would accept a brief presentation from David.
419. Mr David Heatley (Parents' Autism Lobby): I am chairperson of the Parents' Autism Lobby (PAL), which is the parents' voice in the charity of Autism NI. We represent 30 groups across Northern Ireland and a list of them is at the back of the paper I have given to members. Branches vary in size from having only 10 members to much larger groups of over 50 members and a few have over 100 members affiliated.
420. Autism NI has approximately 800 registered families and agencies who are members of the charity. However, all branches also have families who have not formally joined the charity but count themselves as members. They may not have paid their £5 or whatever, but they are associated with the charity. Therefore, I can confidently say that PAL represents over 1,000 families across Northern Ireland.
421. That mandate gives me confidence to back every statement that Arlene has made on behalf of the charity. I have been in regular contact with the branch-support group network by phone and letter over the past year. I have personally visited almost 50% of the groups over the past nine months and I have meetings set up with another five before the end of first week in February. In all my contacts, no parent has said that he or she does not want legislation — not one.
422. What do I hear? Parents ask me why it has taken so long for legislation to appear. Is it not just common sense to see that autism is being left out and that there is a little gap to be filled; and that we need joined-up government so that we do not have to fight the battle with one Department and then separately with another and then another? Parents tell me that services are terrible and that they get diagnosis and are then avoided. After diagnosis, there is no one to help or explain. Everyone is too busy to help, and some of those parents are on their own. Unless you live with autism, you cannot possibly understand.
423. The branches I have mentioned vary from some that are very new, only a few weeks or months old, to some that have been established for many years. Do you know the date when the first one was founded, Arlene?
424. Mrs Cassidy: Yes. The first was established in 1993.
425. Mr Heatley: The expertise in those branches is only surpassed by the expertise and professionalism of the Autism NI staff team. Many of the team are also parents of individuals with ASD. The very first diagnostic training in Northern Ireland took place in 1997. It was set in place by Autism NI and funded by the east Antrim branch. Parents paid for it. Since then, there has been training every year, thanks to Autism NI. In recognition of this, Autism NI was made an honorary member of the Independent Northern Ireland Autism Diagnosticians Forum, a group of ASD experts unique within the UK and Ireland. Most diagnosticians and other experts in Northern Ireland have received much of their training through the charity. Therefore, the charity has led the way right from the very start. Parents are very angry that the 20 years of work, expertise and partnerships that Autism NI has had have to a large extent been overlooked over the past year and half or more
426. Autism NI's lobby campaign started in 2001. It is a founder member of the Celtic Nations Autism Partnership and the Atlantic Autism Alliance. In 2006, Northern Ireland was ahead of Wales in the international autism strategy, but unfortunately politics here got in the way of that progress. Our parents are sadly used to being let down. So much has been promised in the past. Seeds are sown, but the fruit never ripens, it withers on the vine. Please make sure that this is not another blind alley.
427. The autism community needs this Bill desperately. We are being disadvantaged by a disability that is not recognised in law. Parents are already under unbelievable stress because of the very nature of the condition; and it is not only the parents, but the siblings, grandparents and wider family circle, carers and schools. The Bill needs to do exactly what it says on the tin. It needs to be strong and watertight: it must become law. However, if it should fail, we will be back. We will not let this rest, we will just lobby and lobby.
428. Thank you for your time.
429. The Acting Chairperson: Thank you for your presentation.
430. First, I can reassure you that, no matter what I heard earlier, I fully support the Bill and I will not change my mind. Nothing has changed for me. Secondly, you spoke of some amendments. If you want us to see them, we will need to have them in writing before 13 January. Bring them to us and we will talk about what we can and cannot do. Thirdly, I was disturbed to hear that problems were being created over funding. I hope I speak for the Committee when I say that we take a very dim view of anyone in the Department or any other area who plays games with funding because of support for the Bill. The Committee will take a very serious view of that. I hope that message is passed back to the Minister from his official at the back of the room. That is my view on that.
431. I have two questions. Cost is being used as an excuse. Please explain why there will not be a huge increase in cost? Why is the Department so opposed to the Autism Bill? I believe it will complement the strategy that we have already.
432. Mr Callaghan: I think we heard enough on that from the Department.
433. Mrs Cassidy: All jurisdictions find cost very hard to quantify. The analysis behind this document is very revealing. I will make the obvious points. With an effective cross-departmental strategy, with good strong leadership at the head, the potential for cost saving through reduction of duplication is incredible.
434. The issue of training came up quite a bit. There are levels of training, and each Department is accessing training for staff that is very similar and will only increase. A strategic look at training is essential. However, it has already happened. Ironically, Autism NI received funding three or four years ago from the Health Department to look at the development of a training strategy for autism in Northern Ireland. We put that work out to tender, and the University of Ulster completed that document and convened round table discussions across health, education and the voluntary sector. The report was written, but I do not believe that it has been accepted by the Department of Health yet. However, that report sets out an implementation strategy for cost-effective training across Departments, utilising all resources efficiently.
435. My other point is that people with autism are already out there. That is highlighted in Martin Knapp's study. They already cost the nation a lot of money, not necessarily appropriately. Consider the issue raised earlier; misdiagnosis, which may put adults through psychiatric inpatient services, where they receive inappropriate drug treatment when the condition all along is autism. A lot of inherited mental health issues may have stuck to that person because of unmet need. Such a story is not untypical.
436. Ms Paula Hanratty (Autism NI): Cost is a big issue at the moment because of the economy and the cuts. However, there is a massive cost to families, mental health carers and relationships, as well as to the education of an individual with autism, and their ability to work and contribute to the economy. There are massive emotional and physical cost implications for families when parents/carers are unable to work, and they need to be offset against costs that may be incurred.
437. Mrs Cassidy: Paula Hanratty is our director of family support. She is also a parent. Audrey Mullan works for the South Eastern Health and Social Care Trust. She is also a parent.
438. Mr Heatley: I was a school principal, but I had to give up that job because of autism. I could not come home, work with Christopher until bedtime, then work for school and go back next day and cope with the job. My doctor told me that I had to give the job up.
439. My wife ended up with anorexia and spent five months in hospital last year. I was left looking after Christopher. I was also holding down a shop job at the time, but had to give that up. My family's income has disappeared, and I am, therefore, not paying the taxes that I was paying before. Mine is a simple example, but some are much more complex.
440. Ms Audrey Mullan (Autism NI): I did not work for 10 years. Nobody would have employed me because of the number of appointments I had for my son. He has co-morbid difficulties as well as Asperger's syndrome. I had to go to so many appointments, so I understand why parents' incomes are reduced, because they have to look after their children.
441. A lot of money is spent on going to appointments, especially when there are co-morbid difficulties. Therefore, a family's income is drastically reduced, because both parents cannot go out to work, or can maybe work only part time. Single parents find it very difficult to makes ends meet, and, depending on the difficulties, find it difficult to go to appointments at hospitals or with paediatricians. There are huge costs.
442. Mr Heatley: If there is intervention and support, there is a chance that those families could be effective and able to support the community.
443. Mrs Cassidy: It is a huge puzzle to us also why the Department is opposed to the Bill. We are able to multitask as an organisation. We are a very active member of the DHSS action plan and have attended in excess of 40 meetings in the past year. The model is complex.
444. We are also a member of the training and communication subgroups, the reference group, the Western Health and Social Care Trust forum, and the Western Health and Social Care Trust forum subgroup on children. We are not without investment in the process, and we contribute what resources we have. However, we do not believe in a one-Department strategy. Autism requires a whole-life approach; it is a holistic issue. So, we are puzzled by the Department's attitude. I believe that it is a reflection of the silo situation: they are making honest comments about how they see things in their Department but are not able to see that this is about life.
445. Mr Heatley: The key issue when they kept talking about the DDA was that they did not look at it that way. However, they could not see that other Departments do depend on the criteria in the DDA. It is impossible to get supported housing unless one has a learning disability or mental health issue.
446. Mrs Cassidy: We have an active member from west Belfast who has 10 children. If she were here, she would argue the point that a number of her children are on the spectrum, and some have a learning disability and some do not.
447. Children with a learning disability access services through learning disability services. Those with autism, who do not have a learning disability, do not have access to services unless they inherit a mental health problem because of unmet need or if there is a co-morbid condition. One of our other chairpersons has a letter from her trust stating that it does not provide services for individuals with an IQ of over 70. There is evidence.
448. Mr Girvan: Thank you for your presentation. I put on record my congratulations to the group for its tenacity in driving forward and keeping at this. Mention was made of a few clauses in the Bill over which there is some concern. I caution the group against raising some issues, in case that might delay the Bill. The Bill will be of some benefit.
449. During the presentation, there was mention of the bullying tactics of the Department, which is the only way I can describe them. This is not the first time I have heard of that, and not only in relation to autism. The Department is arrogant, and it seems to use the process. Mickey and I attended an event this night last week at which the arrogance of some members of the panel was only too evident. They showed a lack of understanding about their responsibilities. We do not claim to be clinicians or to know the ins and outs of detail, but we know how to manage certain things and make sure that things happen.
450. You talked about how the referral system was used to meet targets. Please explain that to me. However, before we come to that, will you address the issue of cost? Had one listened to the Department's presentation, which was given prior to this one, one would think that it was doing everything and that therefore there would be no cost to the Department at all. I am saying that we are trying to look at the overall picture. It is not necessarily only the pounds, shillings and pence cost that is involved. The quality of life for families is a cost that is suffered and has to be addressed.
451. Perhaps you will give us an insight into the case study you referred to and the testimony you gave of one family and a young chap who had to be sectioned. Was that a recent occurence? If it has occurred while the Department's strategy is supposedly in place and shows how this is being dealt with, that creates a bigger problem for me.
452. Mrs Cassidy: Audrey will answer one of your queries, Paula the other.
453. Ms Hanratty: I will talk about the issue of children being reviewed and referred for assessment.
454. The phrase used is "watchful waiting". A child may go through an initial assessment process in which there may not be sufficient evidence for him to be diagnosed or his condition may tick some boxes, but not all. The normal process is to review in six or twelve months to see whether, as the child gets older, things change, become more obvious, or improve. At the moment, the difficulty is with the number of calls we are getting from parents whose children are being placed in "watchful waiting", yet seem to have a very classic presentation of autism. We are concerned about the numbers. Minister McGimpsey talked about an increase of 40% this year. The numbers going through to try to meet that target are possibly being placed in the "watchful waiting" category, rather than in a more thorough process. So, there are concerns about the quality of placing someone in the "watchful waiting" category.
455. Ms Mullan: You wanted to know about the particular family. It happened very recently. I first met them in April and went out to visit them. I was subsequently contacted through our helpline around four weeks ago. The mother had my name, and I took the call. I referred her to her GP and told her that she needed to follow this up because the child was not well, and that she needed to get a referral back to the GP and get the child's anxiety levels down. She came back to me last week. I spoke to her on the Friday and the events happened on the Monday, but there was a build up as recently as three weeks ago.
456. Mr Girvan: It worries me that we have been told that the strategy is in place and that the programme is working and has been implemented.
457. Ms Mullan: It is also about the process in the hospital. The mother, when she spoke to me last week, said she could not believe that eight psychiatrists had been asked to come and help her by the doctor in A&E, and none came. They had to spend a night in the hospital, which was very distressing for the child because he was in a new environment. He was on the floor crying and they had to spend the whole night there before a psychiatrist eventually came. Even after the child's being sectioned, the psychiatrist still did not come. They hoped that the child being sectioned meant that a psychiatrist would come, but that did not happen.
458. Dr Deeny: Thank you, ladies and gentleman. David, I could not agree with you more. I have seen a number of conditions in all practices. This is a family disease, almost, because it affects everybody, and you have my support. Paul touched on this point, but, one thing that shocked me is the huge increase in the number of sufferers that we are seeing from a clinical perspective. You said that there are 5,000 school-aged children with autism now as opposed to 900 in 2002, and that the ratio has changed from one in one hundred being affected to one in sixty in the past three years. Why is that the case? Is it because of under-diagnosis in the past?
459. Secondly, I will get this in now and then shut up. I think that autism has fallen into the same trap that we talked about before; the whole nonsense of targets. I have had suspicions about targets from the start, both as a clinician and as a doctor. This is all to do with people getting their first appointment. That had to be done within a certain period, and after that, it was a case of to hell with you.
460. I will quote one incidence. However, it is not about autism. Yesterday, I saw a young man whom I know. He is a very pleasant young man in his 30s and has multiple sclerosis. It was the first time I had seen him in months, and I was shocked to see his deterioration. He can no longer manage to climb stairs, and has lost some of the power in his left leg; not completely, but he is walking with a stick. I checked, and his case has not been reviewed by a neurologist for a year and nine months.
461. The same thing is happening here. The phrase "watchful waiting" is a very fancy term that they have given you, Paula. It is a very polite term. It means they have put people on a waiting list, and to hell with them. That is what happens in the Health Service — as long as the first appointment meets the target, they are happy. However, for the review, diagnosis, follow up and care, people are being put on the long finger. Had I not I phoned this morning, God knows when that fellow would have been seen. He will be seen until shortly after Christmas. There were all sorts of apologies and excuses, but I think it is the same thing with autism. You mentioned the re-referral system.
462. Mrs Cassidy: That is really the watchful waiting.
463. Dr Deeny: Do GPs have to re-refer or expedite cases? That happens sometimes. Usually, a phone call asking why my patient is waiting to be seen does the trick. Even in some cases as serious as potential cancers; the first appointment has been on time and then, suddenly, the patient does not know when he or she will be reviewed. It is as bad as that.
464. We have mentioned it before. The Department needs to sort the situation out quickly, because a lot of people with serious conditions, including autism, are waiting for review appointments now. I have been told that the Department is going to look at that, but I do not know how long it is going to take.
465. Mrs Cassidy: As regards prevalence rates; the rate of one in sixty has been quoted by the Belfast Education and Library Board, and we are awaiting confirmation of that. The fact that people such as that are mentioning such figures is worrying. We are no wiser about the cause of the increase in the prevalence rate. As we have always thought, there is a combination of factors such as slightly better awareness and better diagnosis.
466. Mr Heatley: There are more people with it as well.
467. Mrs Cassidy: Yes, absolutely. People feel that the rate of increase cannot be explained solely by better diagnosis, because the resources are not so widely available for it to be the sole cause. We do not know whether the increase is down to environmental factors. Obviously, a lot of work is being done on genetics, so we know that there is a genetic factor in play.
468. Ms Hanratty;
469. I would like to respond to Kieran's point about review after diagnosis. My son will be 18 in February. He was diagnosed in the child and family clinic at the Royal when he was six. He has never been reviewed.
470. Dr Deeny: That is shocking.
471. Mr Heatley: Likewise, my son is 16. He was diagnosed when he was four and has never been reviewed.
472. Dr Deeny: The point that you made, of which we see evidence, is that the first-time appointment target culture that has come into the Health Service means that even the initial assessment is not done thoroughly.
473. Mrs Cassidy: That is the point that I would like to make. I know the diagnosticians involved in this field. A number of them were the pioneers who really linked-in with our branches in the early days and made sure that they got the training and the specialist assessment tools that they needed, such as the Diagnostic Interview for Social and Communication Disorders (DISCO), the Autism Diagnostic Observational Schedule (ADOS), the Adult Diagnostic Interview (ADI), et cetera. They made presentations to their trusts to get resources dedicated to set up the small ASD diagnostic clinics. I know that there is disquiet among them about the quality of the assessment. The informed nature of the assessment is suffering as a result of the target culture.
474. Ms Hanratty: A multi-disciplinary approach is good standard practice. This is becoming less so in the case of autism, as the child may be seeing only one or two professionals rather than the whole gamut.
475. Mrs Cassidy: A diagnostic scoping study was carried out between 1998 and 2002 by the University of Ulster, which laid out examples of best practice. Those examples are being eaten away. The point that I was trying to get across is that a lot of work has been done by us and the health and social care trusts. However, instead of being built upon, that work is being reshaped and redesigned.
476. Mr Heatley: It is such a waste.
477. Ms Mullan: Recently, I received two calls about children who were diagnosed at two-and-a-half years old. Clinicians are extremely good at being able to diagnose now, but the point is that those children will not receive any early intervention until they are three. At that point, they will go on a waiting list, which is six months long. So, people have to wait a year after a diagnosis before they get the early intervention that they require. The child might get sent to speech and language therapy or to occupational therapy, but it is the early intervention that is important in helping the child to learn how to socialise and play. In one case, a mother was told that it will be a year before her child receives any services.
478. Mrs Cassidy: Autism NI has done a lot of work on early intervention, and we are linked in with other groups who are mainly interested in that area as well. There was a particular project on how to get information to parents who are on the waiting list for a diagnosis. It is all there, but it is not being implemented because it has been caught up in the service redesign and the "let's talk about it" attitude.
479. We were already in partnership with Early Years, formerly NIPPA, and Barnardo's in rolling out training to preschools. Instead of grasping that, evaluating it, and, if it is fit for purpose, rolling it out, we have the frustration of planning. I am not saying that planning is not needed: it is needed, absolutely. However, this is about identifying areas of good practice that can be built on while reshaping things.
480. Dr Deeny: We have talked about the need to do something about targets, which are impacting on many issues — and here we go again with autism. It is the same thing. A couple of weeks ago, I said that two patients who came to me had been put off the waiting list. One had phoned to say that he was going to a family funeral, and the other was in the hospital casualty unit at the time, suffering from the very condition for which he was referred. However, because he did not show up for his appointment, he was put off the waiting list. So, the first appointment targets are having an impact across the Health Service, including in the treatment of autism. I should declare an interest as a doctor. Management are pushing clinicians to see people within 13 weeks. If reviews are not seen, management's attitude is "so what", so long as targets are met.
481. Mrs Cassidy: That is it. Multidisciplinary assessment was best practice and it was —
482. Dr Deeny: This is certainly not good clinical practice, at all.
483. Ms Hanratty: As regards the target; if a child is already at school and the family or teachers recognise that he or she has difficulties but do not recognise that the problems may be caused by autism, and that child is waiting see an educational psychologist, the 13-week target does not apply. Because of schools' priorities and the limited access to educational psychologists, it may be several years before the child gets to see an educational psychologist. Therefore, if the difficulties are not recognised as autism, the child's education pathway will become completely different.
484. The Acting Chairperson: I remind members to ask questions that elicit more information on the Bill.
485. Mr Callaghan: My question may be more of a request. As the Chairperson said at the start of the session, I have heard nothing to convince me that the Bill is a bad idea. Luckily for the witnesses, I must be in Drumahoe at 7.30 pm, so I will not take up too much time, since they have been here for quite a while.
486. On the suggestion about amendments to clauses, I agree with Paul Girvan that although the witnesses do not want to accept anything that is substandard they may want to be careful about suggesting amendments without thinking them through thoroughly. In particular, the suggestion about the timing of consultations with Departments is, I think, dealt with in clause 2(1), which provides for an overall two-year deadline for the publication of the strategy after the Bill is enacted. Consultation will have to take place within that two-year period, and anything beyond that will be dealt with as a matter of regulation.
487. Secondly, and as I said in the Assembly debate, as far as I am concerned, the Bill is silo-busting. I and my party's view is that, as the witnesses outlined, the Bill is all about getting Departments to look beyond their own prisms. Pardon the expression, but they are "imprismed" by their own perspective and must move beyond that. A board representative said: "if it ain't broke, don't fix it". The issue is that service delivery is fractured; it is broken.
488. My question concerns the evidence base. It would be helpful if the witnesses would provide the Committee with tangible examples of fractured or scattered delivery in each trust or board area in which there is non-cost-effective duplication. Parents have told me the same thing that Audrey said about the number of appointments, and the more evidence that we have about people having to go to multiple appointments, sometimes to do the same thing, the better. Sometimes being on one appointment list delays getting on another and the person ends up getting referred down the line, and the whole process seems to be all over the place. If members are to support arguments in plenary debates and in dealing with the Department, the more detail that they have the better. That is something that all Members would welcome.
489. Mrs Cassidy: The one amendment, which we heard from the Committee and support, concerns civil servants. An earlier draft of the Bill referred to "public servants", but after advice, it was changed to "civil servants". We would like the phrase "public servants" to be looked at again. It is a matter of interpretation, which is where our expertise ends. We will have to leave that to the Committee.
490. Mr Brady: Thank you for your presentation. It seems to me to be fairly fundamental to the Bill. The previous presentation mentioned a "hierarchy of disability". It seems to me that that was based on the premise that there would have to be a Down's syndrome Bill, and so on. To me, that does not seem to be that relevant. I have represented numerous families since the advent of DLA in 1992. One thing that struck me was that if I represented a child with Down's syndrome, it was a fairly obvious condition. The problem faced by families with children with autism was that it was sometimes very difficult to articulate how the children were affected and how the condition affected their and their family's daily living. A legislative framework, or definition, would, obviously, make things much easier.
491. The impact on families has not been recognised, and that was mentioned earlier. Over the years, I have found that families were affected greatly. David Heatley gave some examples of that, including cases in which carers fell victim to ill-health, even more so than other carers might have experienced. In addition, going back 20 years there have been difficulties with early diagnosis. Mrs Cassidy said that early diagnosis may now become available. I found that children were waiting for three or four years, and, as a result, lost out on early interventions in education and speech therapy and so on. Now, it seems that those children are being diagnosed but are still waiting. We talked about watchful waiting, but children are waiting while no one is watching. That needs to be addressed, because as a euphemism, this situation is like a lot of the nonsense that we sit here listening to week after week.
492. It is the same with the Department for Social Development (DSD). The witnesses mentioned civil servants' training. A civil servant interviewing an adult with autism, who is going to agree, on a particular day, that he could take up the suggested occupation of brain surgeon, is not really addressing the problem. It goes back to what the witnesses have been saying: there must be public awareness, but also awareness that is specifically related to the job that those people are doing. Huge numbers will be affected, and we are only now starting to realise how they are going to be affected.
493. Welfare reform is sanction-led, but we have a Minister for Social Development who says that he will not impose sanctions. I have seen it all before. It is sanction-led, so-called, reform, and the whole point of putting it into operation is to sanction people. It might be held off for a couple of months, but people will end up being sanctioned. People who interview adults with autism, in particular, and young adults must be specifically trained. Lone parents were mentioned. Lone parents with a seven-year-old child or younger are being forced out to work. The objective is that that will eventually apply to lone parents with a one-year-old, but we do not even have a childcare strategy, never mind a proper childcare —
494. The Acting Chairperson: Mickey, is there any chance that you could get to a question, please?
495. Mr Brady: I wanted to raise those points. I am emphasising the need for the Bill. It will not create a hierarchy of disability; it will deal with a specific issue that needs to be dealt with.
496. Mrs Cassidy: We were absolutely insulted when we first heard the phrase "hierarchy of disability" in connection with the Autism Bill and the stance taken by the Department and the board. We have always argued for the existing hierarchy of disability with regard to autism to be removed. This is about addressing a gap —
497. Mr Heatley: It concerns equality.
498. Mrs Cassidy: It is about equality. Just to reinforce what was said about the particular impact; research carried out earlier in the year shows that 80% of mothers of children with autism experience high levels of anxiety, with 50% on long-term antidepressant medication. That is independent research. It is not as though one wants to say that it is more stressful to care for children with autism than those with other disabilities. However, international research is saying that the stress levels of primary carers of children with autism are higher than for any other disability group. That is very powerful. It needs to be double-checked. We double-checked it.
499. Mr Heatley: The research actually included terminal illness, which is hard to believe.
500. Mrs Cassidy: It is incredible to believe that. However —
501. Mr Heatley: It is because autism never stops.
502. Mrs Cassidy: The nature of autism is that it is sustained for life. We have never had to pull those arguments out of our socks until we were faced with the claim that we were causing a hierarchy of disability. We could not believe it. That is far from the case. It is an equality agenda issue.
503. Ms Hanratty: I want to pick up on the point about civil servants assessing people. If a civil servant assesses someone whose hearing is impaired, accommodation will be made to enable that person to have equal access in order to have a full assessment.
504. Mr Brady: By law, someone must have an interpreter if English is not his or her first language.
505. Ms Hanratty: Autism is a social and communication disorder. That needs to be recognised. Additional accommodation needs to be made for individuals with autism to have their rights and an understanding of their difficulties to be supported in assessments.
506. Mr Brady: Alex will agree with me that the Committee for Social Development has asked for exactly that.
507. Mr Heatley: It also concerns policing and justice.
508. Mr Brady: That is why it is such a cross-cutting issue.
509. Mr Heatley: Absolutely. It is good to see how knowledgeable the Committee is about the condition. Members, obviously, have great knowledge about how it affects people. It is very reassuring.
510. The Acting Chairperson: Thank you for your presentation. Before I close the meeting, I wish everyone a happy Christmas and new year.
13 January 2011
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Pól Callaghan
Mr Alex Easton
Mr Tommy Gallagher
Mr Paul Girvan
Mr John McCallister
Ms Sue Ramsey
Witnesses:
|
Ms Grainne Close |
Autism Initiatives Northern Ireland |
511. The Chairperson (Mr Wells): Mr Hanna and Ms Close, I am sure that you are a little shocked that you have been called so quickly. We dealt with other business much faster than we expected to. You are very welcome to the Committee for Health, Social Services and Public Safety, and you are aware of why we are here, which is to discuss the Autism Bill.
512. We usually allow witnesses 10 minutes to introduce the topic, after which there is 45 minutes of questioning. You may have watched or listened to previous evidence sessions, so you know the procedure. We are very keen to hear your point of view on this important legislation.
513. Mr Alan Hanna (Autism Initiatives Northern Ireland): We will keep our evidence concise, and members already have our submission, which I will summarise.
514. I often refer to our organisation as being the largest direct service provider for people with autism but the least well known. We provide services to over 200 families across Northern Ireland and employ almost 250 staff, but people often ask what Autism Initiatives Northern Ireland is. We provide a range of services, mainly to adults, particularly in supported living, residential services, community outreach and floating support. We are very much involved in caring for people who need extensive support. Often, those are people who have been resettled from long-stay hospital, but we also help people towards independence. Floating support is about keeping people in their own homes or preparing them to live more independently by providing support where it is needed.
515. We also provide a range of support programmes to young people. Our youngest service user is around eight years of age, but that is a relatively small part of our work. Our main contacts are with adults. It is striking that much public attention is, understandably, on the areas of diagnosis, young children, families and education. However, all those children grow up and will need support throughout the rest of their lives. That is one of our strengths: we take a more strategic approach to autism because otherwise health could become the provider of last resort. People who could be capable of further and higher education and of competing in the workforce may not get the opportunity to do that, and their services remain largely within health and social care.
516. That gives members some background on the organisation. I do not propose to read through all our submission because members already have it. I will highlight only some areas.
517. We have been strong supporters of the move towards an Autism Bill throughout the process, and we acknowledge the strong support and leadership of Autism Northern Ireland. Autism Initiatives Northern Ireland used to share the same office with Autism Northern Ireland. We carried on the direct service work while our colleagues down the corridor looked after the information and campaigning work. We kept a close eye on that work and have seen it develop over a number of years. We hope that it comes to fruition. There is a strong case for both a legislative and a strategic approach to autism in Northern Ireland, not least because of the numbers involved and the relatively sudden increase in diagnosis and an increased recognition that people have the condition.
518. It is interesting that members referred earlier to the Public Health Agency press statement on swine flu. At this time last year, when we thought that a significant proportion of the population would contract swine flu, we made a number of strategic and operational decisions and actions to prepare for that. In the absence of a legislative process for autism, we have not been able to respond in the same way to a large increase in the number of children and young people coming through the system who will then feed through to adult services in the future. We hold that view strongly.
519. The Minister of Health, Social Services and Public Safety issued an autism strategy last year, and we have been involved with the regional strategy process. We are also extremely supportive of that and do not believe that the Bill and the strategy are mutually exclusive. We are able to push on with a number of issues that would probably be strengthened with legislative backup.
520. I will move on to the main issues that are proposed in the Bill. Firstly, there is a proposed amendment to the Disability Discrimination Act 1995. Grainne and I are not legally trained, but it seems to us that the range of ability or impairment associated with autism is so wide that some people are clearly receiving services through either mental health or learning disability provisions, but there are others for whom access to those services is difficult. That is partly down to a misunderstanding of what autism is. Some of it is also down to the way in which we have structured our services.
521. There is a major challenge for health and social care. If we have a learning disability service for people who have an IQ of a certain level, it is clearly not the service for people with an IQ above that level. If that person does not have a mental health problem, mental health services are not for them. Currently, there is no obvious place for health and social care to respond to those needs. That may be part of the outworkings of either the regional strategy or the Bill.
522. There is certainly evidence that a key part of employment legislation and disability discrimination cases are concerned with the definition of disability and whether or not a claimant is disabled. We feel that an amendment to the Disability Discrimination Act 1995 may help to clarify that position to someone who is not a legal expert. Certainly, it is clear that many people with autism are often recognised as being disabled for the purposes of the 1995 Act, but that is not the case for some people. We think that the amendment would help that.
523. Autism is a spectrum condition, and the range is very wide. In the regional strategy group, a son or daughter could receive a service from an organisation and the staff ratio is 2:1 for that service. Other families in the regional strategy group can describe how their son or daughter is making presentations to their grammar-school class. The range is very wide, and the types of need that arise from that are diverse.
524. We support the autism strategy approach that is recommended in the Bill. We already have the regional ASD strategy. The strongest elements of the Bill will bring other Departments into that. There is a level of co-operation, but, particularly at a time of acute financial difficulty, it is much easier for other Departments to prioritise other areas or reduce services in some areas. A legislative commitment would make it more difficult for that to happen. That is one of the main reasons why we support that approach.
525. As part of the regional strategy, I pay tribute to the work that has already been done, particularly by Stephen Bergin and Lord Maginnis, some of which has been quite controversial publicly. The view that we have taken — and that I have taken partly as the parent of a child with autism, and Lord Maginnis is a grandfather, as well as everything else — is that we recognise the support from other people in the family.
526. As I said earlier, in the absence of a legislative imprimatur, health becomes the provider of last resort. People can find themselves getting into trouble with the law, leaving themselves lost between different services, lacking the support that they need or developing all types of other ancillary problems because there has not been a joined-up approach to meet their needs.
527. Finally, I want to say a little on the collation of data. As I said in relation to swine flu earlier, when we had an estimate of the numbers of people that we thought would get swine flu, we took action. The absence of reliable figures for the actual number of people with autism and their likely future needs means that we have not been as efficient and effective in our planning as we could have been in forecasting the need for employment and training schemes and supported living schemes in the future. There is a disconnect between the time when young people leave school and when they move into adult services. It seems to us that legislation is probably the best way to help that situation at this time.
528. Given the number of people with autism who are coming through the system, and the need to promote even greater joint working between Departments, a legislative approach is probably the best way to supplement and strengthen the work that is under way.
529. The Chairperson: Thank you, Mr Hanna. Ms Close, I presume that you are happy with that.
530. Ms Grainne Close (Autism Initiatives Northern Ireland): Yes, I am.
531. The Chairperson: Many bodies represent autism in Northern Ireland. In fact, it seems that every conceivable angle of the spectrum is covered by a separate charity. It strikes me as extraordinary that so many groups are dealing with the condition in a little place such as Northern Ireland. There is not unity. We had a strong representation from the Aspergers Network, which is totally opposed to the Bill and has great concerns. Why is there a splintering of opinion on the Bill within the sector?
532. Mr Hanna: The range in autism and the service responses are so wide that it is almost not the same condition. Take Asperger's syndrome, for instance: the level of support that we provide to individuals is extremely intensive and is a different experience for many people with the condition. It almost does not feel like the same condition. That is part of it. People become involved in different organisations for different reasons.
533. There are similar disagreements within other disability groups. In a previous life, I worked for another learning disability organisation, and there were divisions within that. People become involved and set up different organisations for different reasons. I am sorry, Chairman; I know that that sounds like a waffly answer. People take different views on issues.
534. The Chairperson: Autism Initiatives Northern Ireland is one of the main providers of care in this field. I am very aware of your work in Newcastle. At a practical level, should the Bill became law in the morning, what difference would it make to the service that you provide? What would you be able to provide tomorrow that you could not have provided yesterday?
535. Ms Close: Alan said that it is a hidden condition for many people on the spectrum. We feel that the Bill would help to identify facts. You mentioned the Aspergers Network. Many of the groups and people with Asperger's syndrome with whom we work do not like to be labelled as having a disability, but the Bill would help us to acknowledge that hidden condition and to be able to support more people with Asperger's syndrome.
536. The Chairperson: Why can that not be done now? The Minister would argue that he has the power to provide funds for any form of treatment or care that is required for anyone on the spectrum.
537. Ms Close: There is an issue about benefits. Some people on the spectrum who would identify themselves as having Asperger's syndrome have difficulty accessing certain benefits such as disability living allowance (DLA), which is a big issue. However, the Bill would help in recognising that there are people with a hidden or invisible condition and that they need help in accessing benefits.
538. The Chairperson: We get lots of letters and cards from folks urging the Assembly to support the Bill. Is there a danger of building up a false sense of hope for those who are treating and caring for people with Asperger's syndrome and all sorts of autistic conditions? They think that there is going to be a revolutionary change, that there will be vast new resources and that many of their problems are going to be solved. However, the Bill is minimalist; it does not promise a lot. Is there a false sense of hope that cannot be sustained?
539. Mr Hanna: The Bill does not specify what individual organisations should do in response to it. However, it strikes me that those people who, with some support, may avoid falling into other services in the future — I am sorry, I am not putting that very well. People with autism who have a learning disability can, in theory, access learning disability services, and many do so. People with autism who also develop a mental health problem can access the services that are run by mental health teams. Our structures do not currently allow for the people who are in the middle, whose IQ is assessed as being over 70 and who do not have a diagnosable mental health problem.
540. I think that the view of those opposed to legislation is that we can simply have a trust reorganisation; that is not a problem. That point — whether we need a law or reorganisation — could be argued for almost anything that comes before the Assembly. We feel that, by giving the issue an impetus through the Bill, structural changes in the trusts could be progressed to provide a service to the people who have neither a learning disability nor a diagnosable mental health problem.
541. If we knew the number of people with autism, that would lead to a more accurate assessment of need. There has to be more detail than simply claiming that there are X number of people with autism in Northern Ireland. The range of need is so wide that it would also be useful to have a notion of how many people are likely to require supported living, will need help to access education and further education in the future, and so on. That is an issue because it is possible to provide services to many people with a relatively small amount of money, at least to those who do not need much support but need some help with co-ordination and activity.
542. We have a staff ratio of 2:1 with some of the people with whom we work. With such people, a staff member has to stay awake with them in their households for 24 hours a day. The collation of numbers and the assessment of need would enable trusts, the Department of Health, Social Services and Public Safety (DHSSPS) and other Departments to plan more thoroughly and cost accordingly for the future.
543. Mr Callaghan: Witnesses have put it to the Committee that, should the Bill be enacted, one potential benefit would be that it would help to reduce the overlap that some people complain about in the provision of services. It seems that there may be disjointed provision between the health side of the house and even various teams working on the trust side, as well as the education provision. The point has been raised that sometimes if a child — or, for that matter, an adult, but I generally hear people talking about children — is in one team, it may temporarily or indefinitely be removed from the influence of another team where it could benefit from certain service provisions or taking up support. What is your assessment of the potential benefits of streamlining service provision to families and people with autism and the wider benefit to the public service generally in efficiency terms?
544. Mr Hanna: A number of years ago, pioneering programmes were set up that brought together further education, education and health, particularly in the area of learning disability. Professionals and parents' groups came together to provide opportunities for people with a learning disability. They were also able to lever European social fund support for that. That would probably not have been possible without bringing those various groups together, otherwise we would have had a disjointed approach that involved someone undertaking an activity that was run by one service on one day and undertaking a different activity on another day. He or she may not have had the opportunity to progress from one to the other. That scenario probably applies more to adult day services.
545. The problem has something to do with the nature of public administration. Some time ago, a special school in Belfast had an issue in that it crossed two health trust areas. The school had therapy support, but one therapist was paid for, for the sake of argument, by the South and East Belfast Trust and the other therapist was paid for by the North and West Belfast Trust. The therapists were not supposed to work with children who lived in the other trust area. A way was found to make that happen. It was not done at a strategic level but at an operational level, and people made it work. The Bill will provide the impetus for such issues to be considered in a more strategic, joined-up way.
546. It is certainly the case that there are some excellent pockets of service in Northern Ireland, but there are some areas in which not much is happening. It is often down to individuals who have made a major commitment and made things happen. It is not a criticism of people in those other areas, but the same set of circumstances has not arisen. There are good services in one place and not-so-good services in others because there is no, or little, strategic approach. The innovation of individuals and family groups made things happen. The potential to spread that across the region would be valuable.
547. Mr Gallagher: I want to ask about the residential facilities that you provide, and particularly the level of demand for those kinds of facilities. What other Departments or agencies are involved with you in that provision?
548. Ms Close: We currently have 92 referrals from the five trust areas. In the Belfast Trust, there are 30 referrals for supported living; in the Northern Trust area, there are 15; in the South Eastern Trust area, there are 45; in the Southern Trust area, there are three; and in the Western Trust area, there are 19. When we receive a referral, we go through an assessment of need with the individual and the family. There is currently a backlog because we do not have the resources to house 92 people, so we will have to set up a priority list. Those are the current numbers for supported living accommodation-based services in the trust areas.
549. Mr Gallagher: Are other Departments involved in that?
550. Ms Close: If 100 referrals have been received by us, some would be from the Probation Board and some from the University of Ulster in relation to helping someone in the college with Asperger's syndrome. However, our referrals mainly come from the health and social care trusts.
551. Mr Hanna: What you may have been looking for is the typical way in which a supported living scheme is set up. We do not run big services. A fairly large ordinary four-bedroom house might house two or three people with autism. The way that that is made to happen is that the house may be owned by a housing association, supporting people through the Northern Ireland Housing Executive, and the Department for Social Development (DSD) would be involved in the funding support for the rent. The Supporting People scheme helps individuals with their support and care costs, and the health and social care trusts are increasingly involved. Essentially, our role is to help all that to stay together by providing support to an individual, but an individual is a tenant in a house, so he or she has a legal tenancy. That has worked very well, but it is clearly coming under severe funding pressures. We have no shortage of potential service users, nor, indeed, does any other service provider out there. There are plenty of people to go around, but perhaps not quite the resources that we would like.
552. Mr Easton: I support having a Bill for autism, and I have yet to hear an argument from anyone about why we should not have it. Why do you suppose that the DHSSPS seems to be so opposed to it? Can you fathom that, especially when the joined-up approach with other Departments that will come from the Bill is fundamental? The strategy for autism is good, but what weaknesses in the strategy could the Bill help to make more effective?
553. Mr Hanna: I can say more about the strengths of the strategy. The number of parents who are involved is important. We found that, when levels of public accountability are raised, standards often rise as well. That applies in this case. When families hear strategic presentations about how things work, they can say that that is not how it works in practice and can challenge that quite strongly. That is something powerful that the strategy groups have been able to bring forward.
554. With regard to weaknesses, the range of disability is so wide that coming up with a service response is quite difficult, because what works for some people with autism probably does not work for others. I am not aware that any assessment was made of the circumstances of the people on the reference group and the regional strategy group. Therefore, there could be many people in that group whose children have very high support needs, which means that they would advocate high support services. However, the opposite could be the case. There still needs to be an assessment of need to understand exactly what the service response needs to be for people with the condition.
555. Our submission states that the practical and direct service issue is of most concern to us. It is because of the practical approach that we have taken that we have not really tried to fathom why other people have taken the views that they have taken. Given that the DHSSPS has had responsibility for this area, it might feel that it will be asked to foot the bill, so it is not quite so keen on legislation. Although the Bill is funding neutral, the result could be an increase in services for people with autism, which is what we want to see. That is also part of the issue.
556. With regard to other — I will not call them weaknesses — areas that could be strengthened, it is still early days for the strategy. Although it has been going for a long time, the meetings can go on for quite a while and people are doing a lot of work, there is much work still to be done. Although the Department of Education is also considering a strategy for its response for people with autism and its relationship to places such as the Middletown Centre for Autism, much more work could be done. There is probably work to be done in further education and training. Although there has certainly been goodwill from other Departments, when they are under pressure for other funding, they can de-prioritise certain areas. Legislation would not allow them to do that.
557. The Chairperson: One point that the Minister might make is that if there is specific legislation for autism, how can it be said to groups that represent people with Down's syndrome or attention deficit hyperactivity disorder (ADHD) that they should not have the same entitlement?
558. Mr Hanna: Part of me would say that that is an issue for those other groups. I do not mean that to sound as facetious as it does. The difference that I see — this is anecdotal — but in a special school classroom 10 or 15 years ago, it would not have been unusual for there to be six out of 10 kids with Down's syndrome. In a special school classroom today, there will be seven out of 10 kids with autism. The change in numbers and in the profile of pupils is such that we would benefit from an approach that allows us to concentrate on autism. That does not deny the needs of those other groups, it is simply that the circumstances have changed and the service response that is required is very different.
559. As an autism-specific service, we have found that, because we try to cater for the specific needs of people with autism, we have service users who have come to us after being placed in other settings with perfectly reputable and good organisations that had not been working in an autism-specific way. Those placements have broken down because of that, and the people have come to us. Although we are far from being a perfect organisation, we feel that by taking that autism-specific approach we have been able to — touch wood — facilitate that and work with those people. What we are suggesting, therefore, is that part of the legislation would be to take that more strategic approach to make those changes for people with autism.
560. The Chairperson: We have received quite a bit of evidence already on the Bill, so many questions have already been asked, which you may be glad to know. In the absence of any other questions from members, I thank you for your time and for your written submission, which has been very useful.
13 January 2011
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mr Pól Callaghan
Mr Alex Easton
Mr Tommy Gallagher
Mr Sam Gardiner
Mr Paul Girvan
Ms Sue Ramsey
Witnesses:
|
Ms Regina Cox |
National Autistic Society Northern Ireland |
561. The Chairperson (Mr Wells): Ladies, you are well known to many Committee members. You have been here before as witnesses and have met us individually on many occasions. However, I formally introduce Regina Cox, who is a co-director of the National Autistic Society Northern Ireland, and Shirelle Stewart, who is also a co-director. You have plenty of experience of giving evidence and know what is expected. I suggest that you take 10 minutes to make some introductory remarks, after which there will be about 45 minutes for questioning. In case you are wondering why the Public Gallery is packed, it is because of the swine flu update that follows your evidence session. They are not all piling in entirely for your evidence.
562. Ms Regina Cox (National Autistic Society Northern Ireland): I thank the Chairperson and the Committee for inviting the National Autistic Society (NAS) Northern Ireland to present evidence on the Autism Bill. I will start by giving members a brief overview of our work, after which Shirelle will talk more specifically about the Bill.
563. The National Autistic Society Northern Ireland is a charity that works throughout Northern Ireland for everyone who is affected by autism, including children, adults and their families. We provide information, advice and support, and we campaign and lobby for lasting positive change for those who are affected by autism. We also have 12 NAS parent branches that provide local support, and we encourage them to fund-raise to deliver local community services such as playgroups and sports activities.
564. Our other services include a help! programme that provides training for parents and carers of children or adults with autism, and a befriending scheme, in which we train volunteers to work with a child or adult with autism and families to provide some respite. We have a parent-to-parent confidential telephone support service and an education advice line. That is popular and provides information, advice and support on education provision and entitlements to guide families through education, which many of them find complicated. We run support groups for parents who have adult children with autism and youth groups for adolescent children. We also have social groups for older adults, who are aged 16 or over, with autism. The linchpin of our services is our team of family support workers who work in the west, the north, Belfast and north Down. Each of those family support workers will support 80 to 120 families over the course of a year and will act as advocates for parents, providing emotional support and, more importantly, practical support.
565. We also have a rolling monthly programme of parent workshops on a range of activities, which are currently free to parents. Furthermore, we provide a range of training for professionals.
566. Ms Shirelle Stewart (National Autistic Society Northern Ireland): First, I will set our comments in context and briefly outline the work in which the National Autistic Society has been involved in autism legislation and strategy development across the UK. In England, the NAS was one of the principal proponents of the Autism Bill, which became the Autism Act 2009. The NAS worked with 13 other autism organisations to take that forward, which resulted in the development of an adult autism strategy in March 2010, and statutory guidance was published in December 2010.
567. In Scotland, the National Autistic Society pioneered the Autism (Scotland) Bill, which is currently in the Scottish Parliament. In Wales, the NAS is an active member of the autistic spectrum disorder (ASD) strategic action plan, which sets out how services will be delivered in Wales. In Northern Ireland, we play an active part in the regional autistic spectrum disorder network (RASDN), which was formed to take forward the Department of Health, Social Services and Public Safety's (DHSSPS) strategic action plan. The NAS sits on the reference group, the adult subgroup and the Northern Health and Social Care Trust ASD forum. The society is also involved in the transitions, interventions and training work streams.
568. I will now deal with specific clauses and our views on the Bill. I will focus my comments on the cross-departmental strategy that is proposed. The National Autistic Society Northern Ireland supports the main objective of the Autism Bill, which is to enhance the provision of services and support to people with autistic spectrum disorder. The society supports clause 2, which requires all Departments to co-operate in the development of an autism strategy and implement any part of that strategy for which they are responsible.
569. Although we welcome the intention for consultation among Departments, we are concerned that the views of people with autism, parents, carers and the voluntary sector will not be adequately considered unless their involvement in that process is outlined in the Bill. With that in mind, we would propose an amendment to the Bill, the wording of which could be along the following lines:
"that the Department should establish a reference group that comprises people with autism, parents, carers and representatives from the voluntary and statutory sector to develop the autism strategy and to oversee its implementation".
570. The NAS supports clause 2, which requires the Department to request that every health and social care trust provides data on the prevalence of autism in its area. That is essential for the planning and commissioning of services. The National Autistic Society Northern Ireland outlined the need for the collection of data in its 'I Exist' report, which examines the needs of adults with autism in Northern Ireland and was published a couple of years ago.
571. In relation to whole-life support for people with autism, the National Autistic Society Northern Ireland supports the content of the strategy in requiring the lead Department to set out how the needs of people with autistic spectrum disorder are to be addressed throughout their lives. Health and social care has started to address some of what we consider historic deficiencies in that sector on autism.
572. In June 2009, Minister Michael McGimpsey published the ASD strategic action plan, which arose from the independent review of autism services chaired by Lord Maginnis. The Minister commissioned the regional autistic spectrum disorder network to take forward the implementation of the strategy, and Dr Bergin and Lord Maginnis head up that process. We believe that RASDN has started to produce some results in health and social care, some of which I will outline for the Committee.
573. The NAS is an active participant of RASDN. RASDN is unique because of the involvement of parents, carers, people with autism, the voluntary sector and the statutory sector, who are all working together to devise services that best meet the need of people with autism and their families. Parents and carers are officially mandated as advisers to that reference group and to each trust. They are involved in all recent investments and in service improvement from the group.
574. A number of things have happened: there was a financial investment in autism services of around £1·54 million over the 2009-2011 period, and a £100,000 investment was announced in November 2010. Although we welcome the investment, the provision of services for adults with autism is negligible in Northern Ireland, so £100,000 is not enough money. More resources will be needed to provide adequate services for people with autism.
575. There has been a reduction in waiting lists for assessment to 13 weeks, and four of the five trusts are seemingly meeting that programme. That figure goes up and down and needs to be monitored, but that is quite a dramatic improvement from a number of years ago when people were waiting for two or three years to start the assessment process. There are also recommendations for the adult diagnostic pathway, which should be coming out in January or February, and work streams are ongoing in training, interventions and transitions. The National Autistic Society Northern Ireland supports the work of that group and suggests that any future strategy needs to ensure that the work is continued.
576. The NAS has proposed an amendment, and we feel that any reference group that is set up should be structured in the same way as RASDN. That is also the policy of the National Autistic Society in that when it devises services or policy initiatives, trustees of the society and board members are elected from parents, carers and people with autism as well as other members of the community. We feel that that is best practice, but it is not common practice in Northern Ireland. We feel that that is very positive and want other strategies being implemented in the same way.
577. I will deal with education because —
578. The Chairperson: We are rapidly running out of time. Is this material in addition to your subamission?
579. Ms Stewart: No, but I just have a little more to say. Educational representatives sit on RASDN but are not officially mandated to do so. That is one reason why we need a cross-departmental strategy. The other reason is that employment and learning are also major issues for adults with autism. The Department for Employment and Learning is not involved with RASDN in a strategic way.
580. I know that the Bill mentions taking cognisance of the health and social care, education and social needs of people with autism; however, I suggest that employment needs to be included, because NAS research shows that only 15% of people with autism are in employment, so that is a major issue that needs to be included in that clause.
581. The Chairperson: If you have missed anything, feel free to tag it on to your answers. Nevertheless, as you might expect, I have to ask you about the elephant in the room. You commented on clause 2, but there has been absolutely no comment from your organisation about clause 1. The obvious question is: why?
582. Ms Stewart: We are not opposed to any amendments to the Disability Discrimination Act (DDA) 1995, but we feel that it probably covers the majority of people with autism. That view is based on training and advice that we have had from the legal profession. We are not lawyers; we seek training and advice. Indeed, the Committee is probably better placed to ask for specialist legal advice in that regard.
583. The Chairperson: That surprises me, because you are one of the main players in the field — a very disparate field — and I question why so many organisations operating in Northern Ireland are dealing with the same condition.
584. Ms Stewart: Look at any other sector. Look, for example, at the environment sector. As you know very well, it involves 14, 15 or 16 organisations. Autism is a spectrum condition, and people are placed at various points on that spectrum. Therefore, the range of interventions that need to be adopted must be child-centred. Another reason why there are so many organisations is that people take different approaches to different interventions, which is right, because a child or adult will need a different intervention depending on his or her need and where he or she is on the spectrum. Furthermore, there should be parental choice so that people can decide what services they need. There will not be a parent in Northern Ireland who feels that the needs of his or her child or adult with autism are being met.
585. The Chairperson: It strikes me as unusual that one of the major organisations in the field in Northern Ireland has not made any comment on an absolutely crucial aspect of the Bill.
586. Ms Stewart: I have just commented. My answer is that we feel that the majority of people with autism are covered under the Disability Discrimination Act 1995. There are also ongoing changes to the Equality Act 2010, which was introduced in GB, and we are out of line with some of those provisions. That is where the Committee probably needs to seek expert legal opinion, because we need to bear in mind the changes that we need to implement to bring us into line with the Equality Act 2010.
587. The Chairperson: That is a very valid point. Nevertheless, it is a bit strange that your organisation, which has many members and is in constant touch with people on the ground who care for people with autism, has not found it necessary to support the change to the definition of the DDA. That indicates that the driving need that others suggest is not there.
588. Ms Stewart: I want to make it perfectly clear that people are being discriminated against. We are not saying that that is not happening, and there is ambiguity in the application of the law by people on disability living allowance (DLA) and employment and support allowance (ESA) tribunals. There is definitely discrimination. We are simply stating what our advice and training has always been. However, that involves the people being discriminated against taking a legal case, which, for people with autism, is a very difficult process.
589. The Chairperson: You cannot feel that strongly about it, because you did not mention it at all in your written submission, and, indeed, had I not asked the question, you would not have mentioned it in your oral submission.
590. Ms Stewart: You cut me short. You told me to finish.
591. The Chairperson: I was carefully following the text from which you were reading, and there is no mention whatsoever of clause 1. You went directly from an introduction to talking about clause 2, and I think that it is telling that there is no unity in the sector about the need for an amendment to the DDA. That comes from my simply asking an obvious question that I had to ask.
592. Ms Stewart: As I understand it, in the context of the Equality Act 2010 in England, changes will have to be made to the DDA, so there needs to be a conversation based on expert legal opinion.
593. The Chairperson: I take it that you have no strong views on the amendments to the DDA and that you are moving on to strategy. Is there anything in the Bill that could not be done without legislation?
594. Ms Stewart: Our view is that legislation underpins strategy. The NAS is a strong supporter of the existing health and social care strategy. However, it does not meet the needs of people with autism across the spectrum in every aspect of their life or provide lifelong support. There is a little bit about health and social care. The Department of Education is developing an education autism strategy, but that needs to come together in one strategy. The Department for Employment and Learning is not necessarily producing an employment strategy. Employment issues for adults with autism need to come together. The Assembly has not produced a cross-departmental strategy. The Bill proposes that it does so, and it compels all Departments to take part in the development of that strategy, which is needed to tackle a lifelong disability such as autism.
595. The Chairperson: There is nothing to stop the relevant Ministers announcing tomorrow morning that they will develop a cross-departmental strategy. It does not require legislation.
596. Ms Stewart: It has not been done, and this is an opportunity to do so. The NAS has been talking about this issue for about four years and has been calling for a cross-departmental strategy since before I joined the society. However, it has not yet been taken forward. The Bill takes it forward, enshrines it in law and gives it teeth to ensure that people co-operate in a meaningful way.
597. Ms S Ramsey: You covered my question, but I will take the opportunity to make one point. I agree with the Chairperson that there is nothing to stop Ministers from coming together to develop a strategy. However, it will involve more than three Ministers. You mentioned DLA. There is a need for supported housing. There is a possible need for the involvement of the Department of Culture, Arts and Leisure (DCAL) to make provision for leisure activities, and so on. Even the Office of the First Minister and deputy First Minister (OFMDFM) should be involved.
598. The Bill puts a strategy into a legal framework. Ministers may introduce a strategy today, but the trusts will not implement it tomorrow. We have seen that it is too easy to cut services for the people who are most in need and most vulnerable. That is a key issue for placing a strategy within a legal framework.
599. Ms Stewart: I agree.
600. In these financial times, it is not popular to say that there has been historic underfunding of autism services in Northern Ireland, and if we want to provide more services, more funding has to go into those areas. From the economic appraisal of the amount of money that it takes to deliver autism services in the UK, it seems that there will be an economic saving as time progresses if we put in place the right interventions and support earlier in a person's life. That would stop us reaching a crisis situation that is costly for health and social care or whatever agency to resolve.
601. The Chairperson: Your group has brought forward parents to individual groups of MLAs and to me as Chairperson of the Health Committee. We learned at first hand the incredibly difficult life that many of those carers lead. Many of them are women, physically trapped in their homes because of the need to care for someone with profound autism. We all get many letters and cards from those folks. Everyone has tremendous sympathy for their situation. However, as I asked the previous set of witnesses, are we not building up a false sense of hope? Many of those folk believe that the Bill, in its own right, will deliver a radical change to their situation. Is that true, or is it not a minimalist Bill that will address some issues but will not provide the resources that they so desperately feel that they need?
602. Ms Cox: We are involved in the regional ASD network. Many of the parents are very committed and give of their time. I have seen that, as time progressed and we started to see results, how encouraged parents are that they can help themselves and make changes to services and have their voices heard. They feel that the legislation will help them to get those services off the ground. As Shirelle says, one of the major problems is funding and getting services up and running, and if that were placed within a legal context, services would improve — not overnight but in the future. RASDN has really encouraged parents in that regard. They have seen changes.
603. The Chairperson: Let us look at the issue practically. You are obviously agnostic on the change to the DDA. However, let us assume that that goes ahead and that, for instance, more children are entitled to DLA. However, the Aspergers Network states that it has been successful in every appeal that it has launched on the issue.
604. Ms Stewart: However, people have to go to appeal and —
605. The Chairperson: Let us assume that a significant number of children receive DLA. Then there is a strategy, and Departments are forced to get together to develop a strategy, which could be six pages stating that a strategy has been developed.
606. Ms Stewart: Legislation is a step on the journey, and any organisation involved in the process understands that. Parents understand that the process takes time. We assume that if a strategy were up and running, there is another job to be done in ensuring that the strategy is fit for purpose. That is the other reason why we suggest an amendment to the Bill in order to involve parents, carers and people with autism as well as the statutory and voluntary sectors in devising a strategy that will be fit for purpose.
607. The Chairperson: Have you floated the idea of your amendment with the proposer of the Bill, Dominic Bradley, and other charities in the field? What sort of support do you feel that you have for the amendment?
608. Ms Stewart: We have proposed the amendment only in this evidence session.
609. The Chairperson: Therefore, you have no idea how the proposer would feel about it.
610. Ms Stewart: No, but it is recognised good practice; I cannot imagine that it would be contentious.
611. Mr Callaghan: I have a few questions; I know that the Chairperson gets a bit nervous when he hears me saying that.
612. I want to make a point that I put to the previous witnesses. There are some issues about duplication and also about a vacuum. To be fair to the Minister, there has been a ramping up of investment over the past years. Partly because of that, I heard one family member say there were times when he could hardly keep up with the number of appointments. There was a feeling that not all of them were necessarily productive, because education authorities were undertaking some activities on the children's side of the house, and people were undertaking other activities on the health side, and they were not necessarily joined up at the top. On the other hand, we hear about people, whether children or adults, who fall outside service provision catchment altogether. It would be helpful to hear your perspectives on that day-to-day experience.
613. Ms Stewart: There is an issue around joined-up provision. Let us take as an example a child with autism who is in mainstream school. That child with autism, as well as probably needing support in the classroom environment, will require speech and language therapy as quite a lot of their difficulties may stem from language. They may also have profound sensory difficulties. It is difficult to provide that spectrum, because there will not necessarily be a joined-up plan. There is no legal obligation on the DHSSPS to provide in a statement the occupational therapy provision or speech and language provision needed.
614. The experiences of children in the classroom and how they cope overspills into the home, so there needs to be joined-up provision between parents and school and school and health. When a child is transitioning into adolescence and adulthood, there needs to be a joined-up approach to getting proper work experience, careers guidance, interview skills and social skills, all of which are necessary to gain employment. At present, the system is not working in a joined-up manner.
615. There is little employment and learning support for people with autism. Many people with autism want to work but do not necessarily have the skills to get through the interview process. Employers do not understand the process of employing people with autism and how to deal with them.
616. Ms S Ramsey: Or benefits.
617. Ms Stewart: Yes, or benefits. That is going through much change, which will cause more problems. People falling through the system has been a historic problem. People with Asperger's syndrome did not fall into the structures around mental health or learning disabilities because their IQ is above 70, so they did not fit learning disability and they did not fit —
618. The Chairperson: The Aspergers Network is the organisation that is most vociferously against the Bill. Does it not strike you as strange that it has put its face totally against it?
619. Ms Stewart: I am not sure what the reasoning is behind that. I am sure that you will ask the network.
620. Mr Callaghan: As the Chairperson rightly points out, the Bill is not a panacea. However, there are advantages to the Bill not being overly specific, because things may change over time. It is ironic that we heard evidence stating that the Department and the statutory bodies want to be flexible in order to respond to changes over time, but, on the other hand, some of the complaints about the Bill are that it is overly prescriptive and constrains people. Somebody must be wrong — I do not know who it is — or is perhaps not anticipating how things go down the line in the correct way. I do not want to jump too far ahead of the Bill, but there is a possible outworking in relation to on-the-ground provision. If there were a unified strategy as prescribed in the Bill, do you think that it would be helpful if there were single assessment points and united service delivery teams? We would then no longer have people working in, for example, an education silo and seeing the educational psychology side. Some of the trusts have dedicated ASD teams, and there is speech and language and whatever else. Do you think that it would make more sense for families who receive services? My examples are more related to children than adults. Is the NAS view that it would make more sense to have cross-cutting teams?
621. Ms Stewart: Yes, without doubt. In order to meet the needs of children or adults with autism we need a multidisciplinary approach. We need to involve people, because the care required to meet the needs of people with autism is extremely complex and involves several Departments as those people progress through their life from birth until death. The only way in which to meet that adequately is through a joined-up approach.
622. Ms Cox: We push for person-centred planning for an individual with autism, so that we are not putting a prescriptive service in place but dealing with each individual child and adult and putting in a service that meets their needs.
623. Ms Stewart: That is extremely important, because one size does not fit all. That needs to be built into any process. A strategy is not written in stone. The legislation compels people to put that strategy together, but it can be reviewed and revised.
624. Mr Callaghan: Over the weekend, I had some conversations with people who knew that the Bill was in Committee. They mentioned the fact, which may not be a disjoin, that certain people deal with children in the school environment and then, when those children go home, they are supported by different statutory officials. It can be difficult for them to provide a properly tailored approach to all of a child's needs, because a school environment can be very different from a family environment, especially for families who might be struggling. Across society, there are some families who struggle and some who have more capacity. It is almost as if a child is dealing with two entirely different environments, which must in itself be quite disconcerting for a child, regardless of whether he or she has autism. Do you have any views on how that type of difficulty could be better addressed?
625. Ms Stewart: One problem that we find is that, when a child goes into the school environment, there is much more routine, but a child with autism often struggles within the environment if he or she is not receiving the right type of support. The anxiety reaches boiling point and, by home time, that child is so full of anxiety that it overspills into the home environment. We also suggest that the right type of support in school would help with the difficulties that a child might experience in the home. There needs to be a plan for a child with autism that looks at the school environment, the home environment and leisure activities, because that child is entitled to the same aspects of life as every other child.
626. The Chairperson: None of the other sets of witnesses really addressed the need to gather statistics on the prevalence of autism. The departmental officials said that they are gathering statistics already. They can improve on that, but their mantra is that we do not need legislation to do that. Where does your organisation perceive deficiencies in the statistics?
627. Ms Stewart: This is probably a new initiative, whereby people are starting to count the numbers of people with autism. In a school environment, one has a better idea of the numbers of children with autism because they have, perhaps, been through the statementing process. As for adults, we have no data to tell us how many adults with autism are in the system. As I said earlier, many of them have fallen through the system. An individual might be registered under mental health services but not necessarily as having autism. Those who have autism and a learning disability will be registered under learning disability services. Those with Asperger's syndrome who do not have either a learning disability or a mental health difficulty have, in the past, not existed. There are many such people out there whose existence the two services do not acknowledge. Many older adults with autism are not known to the services and do not get the services that they need.
628. Ms Cox: Misdiagnosis is also a problem. Adults in their 30s and 40s will have been diagnosed for something else. We must also take that problem into consideration.
629. Mr Callaghan: I will flag an issue. In gathering data, a current difficulty may be that because a co-ordinated approach from departmental level is not cascading down, different data sets are sought. On the health side of the house, clinically diagnosed criteria may be applied, whereas on the education side, criteria may be more based on observed behaviour. We are not necessarily comparing like with like, and that could be a problem.
630. Ms Stewart: You are correct. That data will follow the person from one Department to another. For example, there is no data in the Department for Employment and Learning about how many people with autism receive which benefit or how many people are benefiting. The data is not collected. If someone with autism goes through one of the work programmes in that Department, data is not collected about whether it is successful for that person or whether that programme got him or her into work. Therefore, data is extremely important for the planning and commissioning of services and evaluating which services are the right ones and which support programmes work for people with autism. Data is extremely important.
631. The Chairperson: Thank you very much for your evidence and your answers. Members have all had a chance to ask questions, and we have your written submission.
13 January 2011
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Mickey Brady
Mr Pól Callaghan
Mr Alex Easton
Mr Tommy Gallagher
Mr Sam Gardiner
Mr Paul Girvan
Mr John McCallister
Ms Sue Ramsey
Witnesses:
|
Dr Tony Byrne |
Parents' Education as Autism Therapists |
632. The Chairperson (Mr Wells): I hope I have not caught the witnesses unaware, they are very welcome. I am sure that they have been following the Autism Bill evidence session and are aware of what has being going on. We normally invite witnesses to give a 10-minute introduction on their paper and then allow members an opportunity to ask questions. That normally lasts for 45 minutes.
633. Dr Tony Byrne (Parents' Education as Autism Therapists): Good afternoon. I am Tony Byrne, a father of two boys diagnosed with autism and chairperson of the Parents' Education as Autism Therapy charity, or PEAT for short. With me is Ms Karen Gallagher, the mother of two young boys diagnosed with autism. She is treasurer of the PEAT charity.
634. I first wish to thank the Committee for inviting us to present evidence on the Autism Bill for Northern Ireland. Autism is a terrible disability, and it has a devastating effect on the whole family. My personal position is that my son Conor was diagnosed at the age of two, but with non-intensive applied behavioural analysis (ABA) intervention, he made substantial gains. Conor is now 15, and I am happy to say that he is a normal teenager, although he has teenage problems as all teenagers do, but that makes me happy because he is normal.
635. My son Mikey is a different story. He was diagnosed with severe autism, also when he was two. Mikey needed early intensive ABA intervention, but that was not provided by statutory services. We did what we could for him within our resources, and he made some gains. Mikey is now 13 years old. He still has severe autism. He will never make friends, play football or argue about what time he can stay out to at night with his friends. He will never fall in love or get married. However, we still teach Mikey at home every day, and he continues to make small gains. We love him and we care for him as best we can, but my wife and I always wonder what his life would be like had he received the intensive early intervention that he needed when he was diagnosed.
636. PEAT is the parent-led charity for autism in Northern Ireland, and it was established in December 1997 in response to the non-existent support for families who had taken an informed choice to use applied behaviour analysis to help their children with autism. Our mission is to help such children achieve their full potential by providing parent and care training in applied behaviour analysis.
637. In principle, PEAT agrees there is a need for legislation to protect the rights and interests of persons diagnosed with autistic spectrum disorder (ASD) and their families or carers. PEAT is aware that the health and social care sector already has an ASD strategy, which came about following its review of autism provision, chaired by Lord Ken Maginness. However, PEAT was not consulted in that review, and it raised its concerns about its content when it responded to the autism spectrum disorder strategic action plan produced in 2008.
638. Indeed, PEAT, in collaboration with Queen's University Belfast and the University of Ulster, published a research report in late 2007 entitled 'Meeting the needs of families living with children diagnosed with Autism Spectrum Disorder'. The report focused on families who lived in Northern Ireland, and 100 children, their parents and 67 professionals were subjects of that research. That report was made readily available but was ignored by the Maginnis review and by the strategic action forum.
639. The priority for ASD in Northern Ireland should be effective treatment and intervention. The Health Committee should consider implementing a truly independent review of ASD services that is open, transparent and takes account of international best practice. As a start, I will point out some things that are happening internationally. The Health Committee should look at recent developments in ASD provision in the USA and Canada. For example, Ontario will expand services for children with autism spectrum disorder. Starting next spring, the province will spend an additional $25 million a year to provide applied behaviour analysis services and support in community agencies and centres, schools and homes.
640. In the USA to date, 31 states have passed autism insurance legislation that will require health insurance policies to cover the diagnosis and treatment of autism spectrum disorders. That will also require health insurance companies to pay for evidence-based early intervention, which is widely recognised as applied behaviour analysis.
641. In 2007, the US Department of Defense altered its policy to expand the availability of ABA services to extended care health option beneficiaries with autism. That means if the child of anyone who works for the Department of Defense is diagnosed with autism, they are entitled to early intensive ABA.
642. Applied behaviour analysis intervention is not a statutory right for children with ASD in Northern Ireland. Families must pay privately for such intervention, so it is not regulated. Given the investment and legislation in the USA and Canada, there is a strong economic argument for effective intervention that is based on ABA. Several cost-based analyses have reported on the use of early intervention based on ABA, and all of them conclude that there would be significant cost savings in the long term. For example, Motiwala et al reported that the use of early intensive ABA would reduce the total costs of care for autistic individuals and increase the gains in dependency-free life. Chasson et al, in 2007, reported estimated cost savings in the region of $2 billion for the state of Texas alone if early intensive ABA were funded for existing children with ASD. That is opposed to eclectic provision.
643. There are a number of reports concerning the cost of provision over the lifetime of a child who is diagnosed with autism. For example, Knapp et al, in 2007, reported on the cost of ASD in the UK. The aggregate national costs of supporting children with ASD were estimated to be £2·7 billion each year in the UK alone. Most of that cost is accounted for by services used. For adults, the aggregate costs amount to £25 billion each year, 59% of which is accounted for by services used. That means that, over the lifetime of a child who is diagnosed with severe autism, the total cost of support and provision over their lifetime can add up to around £3 million. However, the cost of an early intensive intervention programme, which will change the life of that child, may cost in the region of £90,000.
644. The recognition of high support costs for ASD is important. Investment in early intensive ABA would reduce high support costs in adulthood. Furthermore, greater availability of effective early interventions may reduce the impact of ASD on the UK and Northern Ireland economies, as well as improving the quality of life for people with ASD and their families.
645. In conclusion, if the proposed Autism Bill will ensure that effective treatment and intervention for children and adults with ASD is delivered in Northern Ireland, it will have the full support of PEAT. Karen, do you have anything to add?
646. Ms Karen Gallagher (Parents' Education as Autism Therapists): Not really. Tony has presented all the points.
647. The Chairperson: Thank you for your evidence. You dealt at length with ABA, which we would expect given the history of PEAT. We are specifically looking at the Autism Bill. Is there anything in the Bill that you believe would mean that children with autism would be more likely to receive ABA than not?
648. Dr Byrne: I do not see anything in the Bill that would mean that children with autism in Northern Ireland will receive ABA intervention as a statutory right.
649. The Chairperson: Do you not see anything in the amendment to the Disability Discrimination Act 1995 (DDA)?
650. Dr Byrne: A case for ABA intervention cannot be taken on the basis of the discrimination legislation as it stands.
651. The Chairperson: That begs the question: why has your group come out strongly in favour of the legislation, if you do not see it making any difference to what you want to do?
652. Dr Byrne: When did we say that we were in favour?
653. The Chairperson: I got the impression from the last paragraph of your presentation that you were supporting the legislation.
654. Dr Byrne: I said "if the Bill would ensure", and that would mean the amendment of the Bill to ensure.
655. The Chairperson: So, you are neutral on the Bill itself?
656. Dr Byrne: We see the issues that are dealt with in the Bill in relation to the Departments of Education and Health, or the statutory services, co-operating as secondary issues. We see the other aspects of the Bill as secondary issues. The priority and real need in Northern Ireland is effective intervention to change lives and make a difference for children and their families.
657. The Chairperson: At the moment, there is nothing to stop the Minister from taking a policy decision that that type of behavioural analysis brings results, and I am sure that we have all seen many examples of such results. You do not require a Bill to do that. That is a resources policy issue rather than a legislative one. There is nothing to stop Michael McGimpsey announcing in the morning what you want.
658. Dr Byrne: No, and there is nothing to stop the strategy in the Bill to help to make those policy changes, is there?
659. The Chairperson: This is not a general inquiry into the level of treatment and care for those with autism; it is about whether this Bill should proceed past the Consideration Stage and become legislation. I am trying to tie down what advantages or otherwise you see in the Bill from your perspective, which is well known because you have been the lead group in advocating that type of early intervention. Many of us would agree that that does produce outstanding results at times.
660. Ms K Gallagher: Surely, when you are formulating a Bill such as this, you have to take in results. It is like a child going to hospital with cancer and somebody saying, "Well, there are good results for chemotherapy, but a bit of this and a bit of that might work, so let's go ahead and try it". When parents are taking an informed decision to go down the route of ABA, which is the only scientifically validated treatment with good results for autism, why should that not be included in Northern Ireland legislation?
661. The Chairperson: That would require an amendment to the Bill, because the Bill does not have any prescriptive care packages. The Bill will be asking for a cross-departmental strategy to be developed for the care of those with autism. It does not, at the moment, say that ABA must be compulsory and given to all who ask for it. The inclusion of that would be quite a radical change to the Bill.
662. Dr Byrne: I agree that the Bill does not say that. We have already had two reviews of autism provision. The Department of Education's review of autism was published, I think, in 2002. There were misconceptions, and evidence on ABA, as the evidence-based intervention that it is, was left out. The Maginnis review, undertaken by the health and social care sector published its findings in 2008. Again, it got it wrong. So, are we going to put two strategies into one that will not address the real issues?
663. The Chairperson: There is a resource issue here. Do we know what it would cost a parent to put their child through a full course of ABA?
664. Dr Byrne: It is estimated at £30,000 a year.
665. The Chairperson: How many children in Northern Ireland do you think would benefit from that type of course?
666. Dr Byrne: We do not have the data. I notice that the Department of Health would have to provide data on how many children are diagnosed with ASD. I know that in the Southern Health and Social Services Board area there may be between 100 and 200 diagnoses per annum. So, a substantial number of children would benefit from early intensive intervention.
667. The window of opportunity is from diagnosis, which should be done by at least two years old, up to seven years old. So, an enormous number of children here could benefit from early intensive intervention. There is also evidence that other children, irrespective of age, will benefit from ABA intervention. In fact, in British Colombia no age limit is set to determine which children can benefit from ABA intervention.
668. Mr Easton: The Bill will result in a joined-up approach between all Departments. That approach is not currently taken. Do you think that that is vitally important to help people with the condition?
669. Dr Byrne: I agree with having a joined-up approach between the two Departments. We are represented on the regional autism network, which is run by the Health and Social Care Board under its strategy. I am aware that the Department of Education will take a similar approach to the development of its strategy. Obviously, those overlap and should be run not in parallel but under the same banner, and co-operation between the statutory bodies is required. If they do not get it right in the first instance and there is a fundamental flaw where they are not following international, evidence-based best practice, they will simply be doing more of the same thing only together.
670. Mr Easton: Some forms of autism are not currently covered by the DDA. Do you feel that the changes to the DDA will cover a lot more of those?
671. Dr Byrne: I agree that some children with Asperger's syndrome fall outside of certain care packages. For example, a person who is diagnosed with Asperger's syndrome may not be entitled to a social worker, and that is totally unfair. I agree that autism is a recognised disability and, whether the person has Asperger's syndrome, another form of ASD — or classic autism, as they call it — it should be dealt with.
672. Mr Easton: Based on those two good points, is the Bill not worth supporting?
673. Dr Byrne: In principle, PEAT supports the Autism Bill, but you have an opportunity to make a difference for the children. We can continue to ignore the evidence. Why would 31 states of the USA legislate to ensure that their health and insurance companies pay for the intervention? Why would Ontario invest an additional $25 million a year in an intervention if it were not worthwhile? Why are children here not entitled to that?
674. Mr Easton: Do elements of the Health Department's current strategy not work well? Does it need to be improved, and is it letting the side down a bit? Are there any areas in which it could be improved?
675. Dr Byrne: Yes, it should go back and look at the so-called independent review, on which it is based. It was certainly independent of any expertise from behaviour analysts, who were not invited to be part of the review. That is surprising as ABA is the intervention that has the overwhelming body of evidence to support it. The strategy should be revisited to ensure that any intervention team that is put in place for a child with autism includes an appropriately qualified behavioural analyst, which it currently does not.
676. The Chairperson: We have had quite a few evidence sessions, so quite a few of the issues have been dealt with already. Is ABA suitable for every child, or are there children who cannot benefit from it?
677. Dr Byrne: The research has been published, and there have been numerous reports on and independent reviews of autism provision. We can forward those many reports to you. They tend to show that 90% of children who gain access to an early intensive ABA programme will make substantial gains. The research shows that 10% of children will make minimal gains, and the reason for that is not known. Fifty per cent of the children will make such gains that they can move to mainstream school unsupported, and you can imagine the benefits that that has for the child, their family and for economics.
678. Mr Brady: So, you are saying that if children do not get the opportunity to have that intervention, you cannot really tell whether they will benefit from it.
679. Dr Byrne: Of course not —
680. Mr Brady: That may sound simplistic, because you gave the example of your two children, one of whom had that opportunity and benefitted and the other did not.
681. Dr Byrne: What I said in relation to my two children was that my older boy's autism is less severe and, fortunately, the provision that we could give him helped him. For our younger child, we spent half our time battling with education boards or whatever. That time was wasted. He should have been put on an intervention programme when he was diagnosed at two and a half years of age, not when he was four and a half.
682. Mr Brady: From my experience of working in the voluntary sector and from talking to parents, I understand that by the time some children are diagnosed, that chance of early intervention has been lost. They might have lost two or three years in which that intervention would have been most beneficial to them. What you are saying makes sense. Is it a resources issue as well?
683. Dr Byrne: Yes, very much so. There are very few appropriately trained behaviour analysts in Northern Ireland, and that is because the investment was never put into training them. PEAT campaigned for the teaching of a master's degree in applied behaviour analysis with specific emphasis on autism at the University of Ulster, and that has been running for several years. It is a part-time degree that is designed for professionals who are already working with children with autism to allow them to become fully trained in applied behaviour analysis.
684. Mr Brady: May I make one more point, Chair?
685. The Chairperson: Is it specifically on the Bill, Mickey? We are drifting away from the Bill towards a wider debate.
686. Mr Brady: A point was brought up about legislation that will affect adults with autism, where it is now recommended that there should be champions or mentors available for interviews and that sort of thing. It is an issue that ties in.
687. The Chairperson: The Vice-Chair will ask a question, which, I hope, will relate directly to the Bill.
688. Mrs O'Neill: Thank you for your presentation. For clarification, are you asking that the Bill should be amended to include the provision that all children with autism should receive ABA?
689. Dr Byrne: Yes.
690. Mrs O'Neill: OK.
691. Ms K Gallagher: That is if the parents wish to go down that route.
692. Dr Byrne: Every child should have the statutory right to access early intensive, effective intervention.
693. Mr Callaghan: My question is very specifically on the first clause of the Bill, on the amendment of the Disability Discrimination Act. There has been quite a bit of consideration of that, and various views have been expressed. Effectively, it boils down to whether the definition of disability under the DDA, as it stands, is wide enough to cover people presenting with autism, so that they get the benefits of protection under that Act. Does PEAT have a view on that one way or the other?
694. Dr Byrne: I really cannot comment. I have experience of the Special Educational Needs and Disability Tribunal (SENDIST), legislation, whereby my child has a diagnosis of autism and, therefore, has a recognised disability. Possibly there are cases where a child has a diagnosis of Asperger's syndrome and is not recognised as having a disability. I do not know. Do you know of any cases where that has happened?
695. Mr Callaghan: To be fair, Dr Byrne, it is not for me to present evidence to the Committee; we are here to gather evidence from people who have direct experience. We are trying to extract as much information as possible from people. A question such as that is designed to decipher whether people can give us practical examples.
696. Dr Byrne: I am not aware of any case of any discrimination case, under SENDIST legislation, where a child has a diagnosis of autism, and that has not been recognised as a disability.
697. Mr Callaghan: Just for the record, the SEN-based legislation is different from the DDA. One is for special educational needs and the other is about disability. The Bill does not seek to amend any of the SEN-based legislation. It is important that that is clear in our minds.
698. Mr McCallister: The Chairperson has told me that I have to mention the Bill.
699. The Chairperson: No, you must "deal" with the Bill.
700. Mr McCallister: All right, I must deal with the Bill. I was going to mention the Bill and then go off on a tangent. If the Bill were to be amended — and you indicated to the Deputy Chairperson that you would be in favour of such a move — do you know what the cost would be? Are we talking about a year's ABA treatment, or longer?
701. Ms K Gallagher: It depends on the child. My son needed a year's treatment, which cost us £30,000, and he sailed straight into mainstream school. It was predicted that he would go into a learning support unit, because his IQ was 75, one point below the learning disability limit. Within five months, his IQ reached 100. He is now nine years old and he has the IQ of a child of 11 years and 6 months. He is coping well at school.
702. Mr McCallister: Therefore, you are saying that if the Bill were amended to include that intervention, there would be an obvious payback.
703. Ms K Gallagher: The payback is there, but, unfortunately, the people of Northern Ireland are remortgaging their homes to provide what they feel are the best pathways for their children.
704. Mr McCallister: In your evidence to the Committee you mentioned an evidence base. Does the NHS provide this treatment in other parts of the United Kingdom? I assume that if this were in the Bill, or if it were provided by the NHS, then those who opt out could be covered, as in the American model, through private health insurance.
705. Ms K Gallagher: The onus is on the Department of Education to provide.
706. Dr Byrne: Unfortunately, in the UK, this is like a postcode lottery. By the time a child receives a diagnosis, he or she is in the education system. Typically, parents will go to their local authority to fund this treatment. In the US and Canada, it falls under health insurance, which is where it is funded. That being said, when children are diagnosed at two years old and younger, it should fall to the Health Department to provide early intervention. Obviously, providing that intervention benefits both Departments, and the average is three years early intensive intervention and anywhere between two and five.
707. Professor Gina Green and Dr Bill Ahern were at Queen's University Belfast on Monday. We were looking at the establishment of an autism research centre, and they are going to help with that. Unfortunately, although representatives from the Health and Education Departments were invited, they declined to attend. Gina has an honorary doctorate with Queen's University and Bill works alongside us. Those people are world renowned experts, and they can give you all the information you want on cost savings and implementation.
708. Mr McCallister: Am I right in saying that unless this is in the Bill you see no huge value —
709. Dr Byrne: I am saying that the priority for children in Northern Ireland lies in effective intervention. The issues being dealt with by the Bill are secondary. Do we want to do the best for our children, or do we want to deal with fallout afterwards, which is what we are doing. The problems arise when we do not intervene effectively, and we have to deal with them. We have to deal with those problems throughout the person's lifetime; not just when they are young.
710. The Chairperson: Thank you for your time, Dr Byrne and Ms Gallagher. We value the fact that you have come along to give evidence and answer questions.
20 January 2011
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mr Pól Callaghan
Dr Kieran Deeny
Mr Tommy Gallagher
Mr Paul Girvan
Mr John McCallister
Ms Sue Ramsey
Witnesses:
|
Mr Dominic Bradley MLA |
All-Party Assembly Group on Autism Secretariat |
711. The Chairperson (Mr Wells): Dominic, we are extremely sorry for the delay. I suggest that members consult the clause-by-clause summary table, which outlines the various concerns raised. As in previous sessions, we will try to take questions on clause 1, then clause 2, and so on.
712. I welcome Dominic Bradley MLA, sponsor of the private Member's Bill, and Arlene Cassidy, who is a member of the all-party Assembly group on autism secretariat, neither of whom are strangers to the Committee. As you are aware, Dominic, the Committee has taken a range of written and oral evidence on the Bill, and the purpose of this session is for members to question you on the concerns that they have heard raised. I suggest that you make a five-minute opening introduction, after which I will allow an hour for questioning.
713. As you can see, Dominic, the Health Committee goes on for an awful lot longer than other Committees — we started today at 11.00 am. I apologise to you and your team for making you sit outside. However, you did not have to; you could have come in and heard some pearls of wisdom about the draft Budget. Nevertheless, I know that you are a busy man and that we kept you waiting for a long time.
714. Mr Gallagher: Had it not been for me, Dominic still would not be here.
715. The Chairperson: Of course, had Tommy not stepped aside from putting his question in the previous session, you would still be sitting outside in the corridor.
716. Mr Dominic Bradley MLA (All-Party Assembly Group on Autism Secretariat): Thank you very much, Chairperson. I thank the Committee for allowing us to make a presentation today and for accommodating the change in time, which is much appreciated. I know that you will have a flurry of figures fluttering around in your heads after the previous session, so I will try to go as easy as possible on you. The Chairperson asked me to concentrate mainly on the clauses, and I will attempt to do that. I made a presentation to the Committee on 14 October 2010, so I will not repeat what I said on that occasion.
717. As the Chairperson said, I am proposing the Autism Bill on behalf of the all-party Assembly group on autism. The fact sheet that Arlene and I provided to the Committee staff earlier illustrates the tension between the unprecedented and rapidly rising prevalence rates of autistic spectrum disorder (ASD) and the limited availability of resources. That, in turn, sets the context for the focus of the Bill.
718. Clause 1 will amend the Disability Discrimination Act (DDA) 1995 definition of disability and insert the words "social (including communication)". It will amend the explanatory list of daily activities to ensure that ASD is included. Practically, for public bodies that use the DDA definition of disability as guidance for decision-making, it will provide more clarity. There is evidence that that guidance is used to make decisions on disability living allowance (DLA), and there is also evidence that school discipline codes result in some pupils with ASD being punished for behavioural reactions that are part of their condition. Clause 1 will, potentially, ensure that ASD must be included in the equality Bill and when compliance with the UN Convention on the Rights of Persons with Disabilities (CRPD) is progressed. For families, the measure will give recognition to a challenging condition that has been low in the hierarchy of disability in our society.
719. When implemented, clause 1 has the potential to cross a range of public bodies and improve public understanding of issues such as access to services and buildings for individuals with ASD. Significantly, it will signal the beginning of the end of discrimination against individuals with ASD who have an IQ of more than 70. For families, the Bill will make a practical difference through the systematic education of the public that will flow from the adaptations to public spaces and facilities. The fact that ASD will be recognised in law will bring a level of validity to a condition that is still treated with suspicion and ignorance by some professionals and agencies. The practical benefit of clarity in law will guide decision-making on benefit entitlement, help to update disability action plans for public bodies, improve access to equality legislation and ensure automatic inclusion in the Convention on the Rights of Persons with Disabilities compliance. Families will have a reference point for service entitlement, particularly for those with an assessed IQ of 70 or higher. The physical adaptations to public buildings will assist not only people with ASD but the wider disability community.
720. I will move on to clauses 2 and 3 —
721. The Chairperson: Dominic, if it does not interrupt your flow, it would be helpful to proceed on a clause-by-clause basis. To keep some sense of discipline, we have been breaking the discussion into three areas: clause 1, strategy and other points. We received a briefing document on clause 1, and we are, therefore, particularly keen to ask you questions on that, especially before we lose our quorum.
722. Mr D Bradley: As far as possible, I will try to do that. I structured my presentation on a clause-by-clause basis, rather than on the finer subdivisions.
723. The Chairperson: Have you finished your evidence on clause 1?
724. Mr D Bradley: Yes.
725. The Chairperson: Do you mind if we ask questions on that before you move on?
726. Mr D Bradley: That is perfectly acceptable.
727. The Chairperson: We received a research briefing from Tim Moore. I do not know whether you have had the advantage of seeing that.
728. Mr D Bradley: I have been briefed on it.
729. The Chairperson: Have you not had a chance to read it?
730. Mr D Bradley: I have read some of the background material elsewhere.
731. The Chairperson: You are aware of his comments that, as an unintended consequence, the Bill could weaken the DDA and that the inclusion of the word "social" could lead some people to believe that other conditions should be included. One view is that the words "mental" and "physical" already cover everything and, therefore, protect those who have autism at any end of the spectrum. Indeed, an industrial case, Hewett v Motorola, shows that to be true in case law. Given the danger that your case could be weakened by its inclusion, are you still minded to have "social" added to the DDA?
732. Mr D Bradley: We are aware of the point made by the Assembly researcher and of his reference to William Hague's letter and to the Motorola case. We are perfectly prepared to examine the consequences of that and, if necessary, to withdraw the second part of clause 1. We would be interested in ensuring that the list of daily activities includes all aspects of ASD. However, at this stage, given the evidence of the researcher and other information that we have, we are willing to consider the withdrawal of clause 1(2).
733. The Chairperson: It is extremely helpful that you are considering that rather than allowing the issue to cause conflict between the Committee and the proposer. I am aware of the evidence of the Equality Commission, which seems to suggest that it cannot ascertain from evidence that the present definition of the DDA precludes worthy applicants from receiving benefits from the Social Security Agency. In other words, the problem seems to be an inability, at times, to argue the strength of the case rather than of proving that the person is autistic per se. From my experience, I know children who receive DLA and children who do not. The argument is not whether ASD is defined in the Disability Discrimination Act 1995 but whether the tribunal will accept that, for example, the person requires a greater level of care or cannot walk more than 50 yards unsupervised. How do you react to that information from a respected body in the field?
734. Mr D Bradley: I do not know where the Equality Commission carried out its research and why it cannot obtain that information. As a working public representative, I have seen evidence that the Disability Discrimination Act 1995 has been used as a means of excluding people with ASD from access to benefits. I will ask Arlene to provide more detail on that.
735. Mrs Arlene Cassidy (All-Party Assembly Group on Autism Secretariat): We have evidence from one case that we are allowed to submit to the Committee of the DDA's definition of disability being used by a decision-maker in a judgement on the receipt of DLA. However, it may be a matter in which the policy states one thing and the operation does another. It may be that there is a deficit in the training of policy officers. That point is also addressed in the Bill.
736. Mr Easton: Today, other witnesses stated that clause 1(2) would narrow the scope of the DDA and that, as a result, people with other conditions would lose out. Personally, I do not agree, but how do you counter that argument?
737. Mr D Bradley: As I said to the Chairperson earlier, in light of information that we received, we discussed that earlier today among ourselves. We were briefed about the Committee's presentation from the Assembly's Research Services. We accept that that is a possibility and, if there is a danger that it would have that effect, we are willing to consider its withdrawal. Do you have anything to add, Arlene?
738. Mrs Cassidy: The spirit of the Bill was intended to be inclusive, but we seem to be caught on the horns of either having minimalistic legislation or including everything. However, with regret, I support the conclusion that Dominic has reached on that issue.
739. The Chairperson: From a procedural point of view, we need that view from you in writing by next Thursday, when we will formally agree a position on the Bill. Although you have been recorded by Hansard as having said that, we need a piece of paper as well.
740. Mr D Bradley: We were made aware of that earlier, and we can provide that.
741. Mr Easton: I agree that some children lose out on DLA. I am dealing with such a case, and I just wanted to back up that point.
742. Ms S Ramsey: The group has taken a very mature approach. Arlene said that the group did so with sadness, but it is a question of building on what is there, and it can grow. As Dominic said, there seems to be, unfortunately, a split, despite everyone wanting the same outcome.
743. You mentioned the issue of the DDA and the Equality Commission. I am a bit concerned that, in light of the evidence, a public body did not reach the same conclusion as we did as elected representatives, community activists and groups. However, I am also concerned that we should not focus the issue of DLA solely on children, because the Department for Employment and Learning, for example, accepts that it must retrain staff working in jobs and benefits offices in the questioning of people with autism. Other Departments have noticed issues and taken action. That issue must be included.
744. The Chairperson: Members have heard what Dominic said, so does anyone have a new angle?
745. Mr Callaghan: Yes. I accept what Dominic said. In coming to that decision, what consideration was given to the fact that the paper from Research Services — I accept that you have not seen the whole paper, and I do not know on which parts you were briefed — highlights the fact that the guidance in England would support clause 1(3)? Some people raised issues about clause 1(3) as well. Is it your intention, Dominic, to retain the part of the amendment to the DDA contained in clause 1(3)?
746. Finally, there has been much talk about the Equality Commission. I have nothing against the commission; I used to work for it. However, as with than any other body, the commission can make a judgement only on the information that it receives. The Human Rights Commission argues in favour of clause 1(2), which you are considering removing. Therefore, how did you balance your consideration of whether to let it go or retain it?
747. Mr D Bradley: As I said, we met earlier today to discuss that. We receive our own advice, and we considered it seriously. As Arlene said, in light of the advice, we are, perhaps unwillingly, prepared to look again at clause 1(2). However, we are minded to retain clause 1(3), because that would become part of the list of daily activities, and it is important that we retain that.
748. Mr Callaghan: The convention, which the research paper references and to which the UK Government and, presumably, other European Governments are signatories and have ratified, specifies the word "sensory" as distinct from the physical and mental. Sorry, I will let that go, because I have lost my train of thought, and there is no point in pursuing it.
749. Ms S Ramsey: It is a matter of getting the Bill through or not.
750. The Chairperson: We will move on to clauses 2 and 3, and I will start the ball rolling. Dominic, we have heard from many witnesses, and there is a huge split between the various groups involved in autism. The views range from being enthusiastically in favour of a cross-departmental strategy to those who think it an absolute waste of time. I have never seen such a variation in evidence from people in the same field.
751. Implicit in the Department of Education's evidence is that it is not bowled over by the proposal for a cross-departmental strategy. This morning, officials made it clear that the Department considers that it has enough power to do whatever it wants in the field. It is of the view that large-scale co-operation already happens and that, legislatively, nothing holds anyone back from what they want to do. They do not see the logic of having legislation to enable something that already happens, and they said that Departments co-operate and meet regularly.
752. Ken Maginnis made the same point and questioned the need for legislation. It is only fair to mention that, given that such evidence was given time and time again by various people, including some autism charities. The written submission from the Aspergers Network was vociferous in its opposition to the legislation. How do you react to that?
753. Mr D Bradley: The all-party Assembly group on autism was briefed by the Health Department and the Department of Education on the same day in the same room. I asked pointedly about the level of co-operation between the two Departments, and, if my memory serves me correctly, the Departments' response was that they met for coffee from time to time. That does not indicate a high level of co-operation between two Departments seeking to co-ordinate strategies that should be integral to each other. There does not seem to be any structured co-operation between the two Departments, and the Bill hopes to achieve such co-operation. Although there is a strategy in the Department of Education and a strategy in the Health Department, my strong impression is that there is not the structured co-operation between the Departments that is necessary.
754. The evidence from the Department of Education officials seems to be slightly at variance from the view of the Minister of Education, who wrote to the Committee for Education in support of the Autism Bill. We should, perhaps, place more emphasis on the Minister's view than on that of her officials, because she is the person who is responsible for the Department. Other Departments are named in the Bill, and they also have a role to play in contributing to the provision of autism services. Autism is a lifelong condition that requires a lifelong strategy. We will achieve that only through the highest level of co-operation possible between all of the relevant Departments. It is my view that that would be best achieved through the strategy that is outlined in the Bill.
755. The Chairperson: I will read three comments. The Parent Carers' Council on Disability said of an autism strategy:
"It would be a waste of resources which could be spent to help and provide services for all families with disabilities."
756. The Equality Commission stated:
"the Commission is not convinced that there is a clear need for the DHSSPS to be placed under a duty to prepare a strategy on autism."
757. Aspergers Network said:
"This Bill has caused huge divisions; and not only with Autism families; but also within the disability world."
758. Those are three players in the field who have a totally different view, and that is what the Committee finds so difficult. Some autism groups are extremely keen on an overarching, cross-departmental strategy, and others from a similar background, including the Equality Commission, say that it is not needed. Why is there such a lack of unity in the field?
759. Mr D Bradley: It is not always possible to achieve total unity, but the all-party group consulted widely on the Bill. On a previous occasion, we provided you with the results of that consultation, and between 70% and 80% of responses to the Bill were positive. We consulted Professor Brice Dickson from Queen's University. Originally, he was dubious about the Bill, but, after we discussed in detail its various aspects with him, he changed his position and became supportive of it. The majority of autism charities and disability groups have no issue with the Bill. The majority of autism charities and voluntary groups, with the one exception that you mentioned, are in favour of the Bill. The evidence, therefore, is that a majority of opinion is in favour of the Bill. I accept that some people are not in favour, but, as I said, it is impossible to achieve total unity on every issue.
760. The Chairperson: We have just heard from Lord Maginnis, who, as you know, carried out a major review on the issue. With him were two parents of autistic children, and they made it clear that the Regional Autistic Spectrum Disorder Network (RASDN) was totally opposed to what you are trying to do.
761. Mr Easton: On a point of order, they said that RASDN was neutral.
762. The Chairperson: If that was neutral, Alex —
763. Mr Easton: That is what they stated.
764. The Chairperson: They said that RASDN was neutral, but, for the next half-hour, I listened to them opposing the Bill.
765. Mr Callaghan: It is also fair to recollect that they said that there was a variance of opinion in RASDN.
766. The Chairperson: They did. However, the last half hour or their presentation left me in no doubt of their total opposition to the Bill. The Hansard report will show that to be the case. At least, Lord Maginnis and the two representatives who were with him were opposed; perhaps that is a better way of putting it.
767. I wish to clarify what you said about the Department of Education. In the Minister's letter to the Committee, she said that she had supported your Bill at Executive level but had then gone out to consultation on the implications for her Department. From the evidence of the departmental officials, it is clear that they are working away in the field and have done so for years. When asked by several members of the Committee whether they could think of one aspect of their work that was hindered by lack of legislation, they said that there was absolutely nothing. They said that the issue was not legislation but one of resources and, perhaps, policy. I am simply throwing out difficult questions to you, as I did to your opponents. Even the officials from the Department of Education, whose Minister supported the Bill, were not enthusiastically behind the need for legislation.
768. Mr D Bradley: It does not surprise me that the group that gave evidence earlier is opposed to the Bill. I have been aware of its opposition for some time. Indeed, Lord Maginnis, as you mentioned him by name, was opposed to the Bill before he even saw it. I do not know on what his opposition is based, but one must question an attitude of opposition to something that a person has not even seen. Regardless of what was in the Bill, Lord Maginnis would be opposed to it, because he was opposed to it before it was even drafted.
769. The Chairperson: Quite a few members wish to speak. Kieran, who has been extremely patient, is next.
770. Dr Deeny: Thank you, Chairperson, Arlene and Dominic. The decision to reconsider clause 1(2) is a wise one. As I mentioned earlier, I chair a group for people who are sensory impaired. People in that group feel that they have been hard done by, compared with those people who are physically impaired, in getting access to the Health Service and GPs. They feel that their needs are being met under the day-to-day activities that you mentioned, Dominic.
771. Dominic and Arlene, you are committed to the strategy, and, as I have been a doctor for 30 years and a GP for most of that time, I have done a great deal of work with people with disabilities, including autism. In fact, I know three of my severely autistic patients very well, and two of their fathers are friends of mine. As I said earlier, we must ensure, not only in health but in education and in legislation, that we do all that we can for all disabled people.
772. I showed the Bill to one lady, and she picked out clause 3(1) and clause 3(3). I am concerned about those subsections. We want all disabilities to be treated well. Is there a potential for, as appeared to be the concern in Scotland, a hierarchy or a prioritisation of disabilities? That lady said that the Bill's provisions for setting out the needs for people with autism were fine but that it would be nice if we could say the same for people with cerebral palsy. Her daughter is in her 20s and has very little use of one side of her body, and many of her needs were not met as she was growing up. Clause 3(3) also refers to the needs of families, which that lady also mentioned.
773. That was the view of one individual, but is there not a danger that people with other disabilities will say that they also want a Bill? We are all here to try to ensure that we do the best for patients across the entire autistic spectrum. However, we must also consider whether the Bill will have any impact on other disabilities, because as a GP I try to meet the needs of every patient with a disability. Someone mentioned disability-specific legislation. Is this the first time that legislation has been drafted for a specific disability?
774. Mr D Bradley: I do not think so. As far as I am aware, the DDA mentions certain disabilities. On the question of creating a hierarchy of disabilities, the Department of Education already has an autism strategy, and, not only that, there is a centre of excellence for autism at Middletown. The Department of Health, Social Services and Public Safety also has an autism strategy. Therefore, those two Departments already recognise that specific action is required to meet the needs of people with autism. The Bill seeks to ensure that the existing efforts, and the additional efforts that are needed, are co-ordinated in the most effective way. In that way, resources can be used as efficiently and effectively as possible, especially when resources are scarcer than in the past. Special consideration has already been given to autism by the two Departments. I will ask Arlene to comment.
775. Dr Deeny: Before you do, I make the point that people with other disabilities might say that there is a law to ensure that people who suffer from autism and their families are looked after throughout their lives and that their needs are met, but that there is no law for their child, who has, for example, Down's syndrome, cerebral palsy or muscular dystrophy. Will the Bill create a problem in the disability community in that autism will be seen as being favoured by the introduction of legislation solely to meet the needs of people with ASD?
776. Mrs Cassidy: The Autism Act 2009 in England already sets a precedent, although it is very different from what this Bill proposes. This is a single disability Act in England. The situation is difficult for people who have disabilities that are hidden, invisible or tend to fluctuate. Special measures were taken, as highlighted in the evidence that was presented this morning by the Assembly's Research Services, to amend the DDA to recognise MS and HIV and to accommodate the difficulties that are faced by people with specific disabilities.
777. Throughout the period of lobbying, a number of conditions were quoted. Dr Deeny mentioned cerebral palsy as an example. To a certain extent, physical disabilities fall into the main mental and physical disability categories. We have met representatives of Disability Action. Many of us who now work in autism worked professionally in the general disability sector before specialising. The last thing that anyone round this table wants to do is to prioritise one disability over another. However, autism is a matter requiring special attention, and we have met representatives of Disability Action, the Equality Commission and the Human Rights Commission. There is unanimity that the Bill will bring clarity and that it is a matter for special attention. The submission from the Human Rights Commission highlights that.
778. Mr Easton: May I raise the issue of cost?
779. The Chairperson: That is the next topic; we are still discussing the strategy.
780. Mr Easton: The one element of the Bill that I particularly like is the fact that it will force all Departments to take a joined-up approach. Despite Departments saying that they speak to one or two agencies here and there, that joined-up approach is lacking. Do you not consider that that element alone merits the Bill's going forward?
781. Mr D Bradley: Yes. I agree with you that government and government services are more effective if they are joined up rather than delivered from separate silos. The purpose of the Bill is to ensure that those services are joined up and are available to people with autism throughout the course of their lives. The Bill will guarantee that people with autism receive the services that they need and that the trauma of major life transitions, which are particularly problematic for people with autism, is lessened as much as possible. That will be one of the major advantages and achievements of the Bill.
782. The Chairperson: I remind members that this is a chance to test the witnesses rather than to issue declarations of support. We will have an opportunity next Thursday to discuss the Bill, and, if members are in favour, they can speak passionately for it then or, indeed, against it.
783. Mr Callaghan: You have taken the wind out from under my sails, Chair. I want to touch on the duty to co-operate. Dominic, I do not know whether you are aware that, prior to Second Stage, the Department of Health, Social Services and Public Safety provided an informal briefing to the Committee. I think that is an accurate recollection to say that the Department stated that it did not have a clue what was contained in the Department of Education's strategy. When we probed the officials on that, they defended that utterance by saying that that was because the Department of Education was developing its strategy, and, therefore, it was not a deficiency on their part that they did not know about it. Is the point of the duty to co-operate not to become involved at an early stage? Much of what they said was about the strategy creating bureaucracy.
784. The Chairperson: Is this a critical question, Pól?
785. Mr Callaghan: What do you have to say to that?
786. Mr D Bradley: If one Department already has a strategy in place, other Departments should use that to implement the lessons that have been learned from it. Other Departments should further ensure that the necessary linkages between the various aspects of the two strategies are made, and those linkages should be made early and should be effective. That type of co-operation is extremely important from the point of view of cost, because, through close co-operation, Departments can avoid the duplication of costs, which may exist currently in education and health. An effective, joined-up strategy can help to reduce costs rather than add to them. That is an important consideration, as we are all aware at this time.
787. Mr Callaghan: As I am sure you are aware, the Committee is caught in a pincer movement. Some people come at us saying that the Bill is far too much and will create undue bureaucracy, and, equally legitimately, other people say that it is not enough. One of the issues raised as a criticism of the Bill's not being strong enough is that the Department of Health, Social Services and Public Safety is designated as the lead Department, but what happens if another Department fails to honour its commitments in the strategy? Clause 2(7) states that the other Departments "must co-operate", but what is the sanction for not doing so? Is the sanction that the Minister for Health, Social Services and Public Safety tables a report to the Assembly as part of a review, as set out in clause 2(9), or is it envisaged that there will be some other mechanism through the Executive or otherwise?
788. Mr D Bradley: Clause 3(6) gives the Department the power to "make regulations" in relation to the "content of the autism strategy." That is a strong power that enables the Health Department to ensure that other Departments co-operate with it in the implementation of the strategy. Originally, we envisaged having an autism commissioner as part of the accountability mechanisms. However, after discussions with various people and in light of the harsh economic times in which we live, we considered that the cost might have negative implications. Therefore, we designed the accountability mechanisms around those that exist currently, which include this Committee and the Assembly. The Bill places a requirement on the Department of Health, Social Services and Public Safety to report every three years on the implementation of the strategy. Therefore, as well as the power to make regulations, Departments will be answerable through that triennial report to the Assembly. That will give a strong impetus to ensuring that Departments live up to the regulations that are initiated by the Department of Health, Social Services and Public Safety and to the duties that come with those.
789. Mr Callaghan: Finally, I will ask you an unfair question, but if you were to have an answer, it would be constructive. The Department says that work is going on at official level, such as at ministerial level and at sub-ministerial working groups. It states that clause 2 will give rise to additional costs for the review, monitoring and implementation of the strategy, as opposed to the resulting services, which are covered in clause 3. Has anybody been able to ascertain how much money is spent currently on the various autism-related strategies? What would be the cost differential in having a single, streamlined integrated strategy?
790. Mr D Bradley: There is a report titled 'Autism: The Costs'. Arlene is very familiar with that, so I will ask her to respond.
791. Mrs Cassidy: Before I do, my understanding is that several Assembly questions on that point are pending. There is a freedom of information request about what proportion goes into administration in the current system and what goes into services, but it has not been responded to. I do not have the answer to that, but I would be interested in finding out, as we all would.
792. The report was submitted for consideration by Autism NI/Parents Autism Lobby at the evidence session. It contains some analysis, but focuses mainly on what it costs society not to provide services.
793. Mr Callaghan: For current purposes, that is more relevant to clause 3 in so far as —
794. The Chairperson: Yes, but I do not mind your drifting into that area.
795. Mr Callaghan: Will we leave that point for our discussion on clause 3, Chair?
796. The Chairperson: OK.
797. Dominic, have you seen the letter from the Minister of Finance and Personnel dated 17 January on the issue of cost?
798. Mr D Bradley: No.
799. The Chairperson: It is very short. It states:
"I wrote to the Health Minister in November 2010 supporting his position on this Bill. I share Mr McGimpsey's concerns particularly about the lack of information on costs and the absence of a finance clause taking account of direct and wider impacts on funding. Given that I do not believe this Bill is needed at present I will not be offering amendments. This response has been copied to the Health Minister."
800. The Bill states that there will be no significant costs, but, this morning, Dr Briscoe said that even the training of 25,000 civil servants would cost £1·8 million. You say that the Bill has no significant costs, but it calls for civil servants to be trained in dealing with people with autism. How does that square with what you are saying?
801. Mr D Bradley: I presume that some of that cost is already being met by the system, because public servants in the Department of Education and the Department of Health, Social Services and Public Safety already receive some autism training. A level of training is probably provided by other Departments, such as the Department for Social Development, although that may not be sufficient. That might be the global figure for the overall costs, but, as I said, some of that is already being incurred by Departments. There may be an extra cost, but it would not be at the level of £1·8 million.
802. Mrs Cassidy: In any case, that cost is inevitable, because the prevalence of autism, including among adults, is rising. It is a question of planning for the future progressively year on year. The cost appears frightening when presented in that way.
803. I support Dominic's point about the training that already happens. Certain disability organisations are involved in training, and those contracts are already in place. The point is that autism should be included in that training, so it is a matter of tweaking existing practice and making sure that autism is not excluded. As with everything, it is all about the implementation. With common sense and good strategic heads, I have no doubt that those costs can be tackled.
804. The Chairperson: Why does the Bill state that training will be for "Civil Service staff" rather than for public servants?
805. Mr D Bradley: That is a good question, and I am glad that you raised it. It has been raised with us by others, and it is a possible change that we will consider making to the Bill.
806. There are financial costs, but we do not believe that they are huge. However, if the Bill were not to progress, there would be a huge human cost to people with autism, whose needs, heretofore, have not been met. Therefore, although there will be financial costs, there will also be a huge human benefit for people with autism, whose quality of life, throughout its various stages, will be improved by the provisions in the Bill.
807. The Chairperson: That brings me neatly to a fundamental point. We have been lobbied massively on this matter, including through e-mails and cards — I received more postcards on this issue from your organisation and its friends than I have received birthday cards in my life. From speaking to many groups, the common theme is the sense of frustration, particularly among those who care for autistic children, about the lack of delivery of services to meet their needs. We accept that that frustration is prevalent throughout the country. Some people say that they want us to support the Bill, because they think that it will solve that problem. I wish that life was as simple as that. There may be some false expectations because, as the Health Department officials said to us today, the Bill does not contain a mechanism to force service delivery. It includes a mechanism to force the delivery of a strategy, but it will not guarantee that Mrs Smith, who looks after autistic children, will receive the services that she clearly and desperately needs. One of my questions, and, strangely, the Department made the same point, is why did you not seek to include something more specific in the Bill to force more than a strategy?
808. Mr D Bradley: The idea behind the strategy is to deliver efficient and effective services to people on the ground. The strategy will be a framework. In a private Member's Bill, it is impossible to be totally prescriptive about what a strategy will deliver and how it should be delivered. If we were to do that, we would end up with a huge Bill that would take the Committee longer than it has allotted to deal with this one. In legislation generally, it is not the practice to deal with every aspect of a service. We have to leave it to the professionalism of people in various Departments to formulate those for themselves. As I said, the Bill contains an accountability mechanism, and, if services are not being delivered, Departments will have to answer to the Assembly.
809. The Chairperson: You could end up with all the Departments getting together to produce a strategy that gathers dust or is utterly meaningless because it does not improve service delivery. The Assembly might criticise Departments for that, as it does in other fields, but I do not know what could be done beyond that. The point was made that the English Act contained a mechanism to improve service delivery, particularly to parents. You might continue building up a head of steam, which everybody thinks is wonderful, and you might have a party when you get your Bill through. However, on the ground, real improvements might not be delivered to those whose home situations have tired them out. There are people who can no longer cope and cannot get respite care or any form of home help. That is the danger of a Bill that does not deliver anything concrete beyond a document in two year's time.
810. Mr D Bradley: Clause 3(3) states:
"The autism strategy must set out how the needs of families and carers of persons with autism are to be addressed."
811. The Chairperson: It sets that out, but it does not say that it has to be done.
812. Mr D Bradley: It is certainly implied that it has to be done.
813. The Chairperson: I suspect that the phrase "subject to the availability of finance", which is the get-out clause in all such matters, will appear somewhere in the strategy.
814. Mr D Bradley: There is no 100% guarantee with any strategy or Bill. We have gone as far as we possibly can in the Bill to ensure that the services delivered will be efficient and effective, but there can be no 100% guarantee. The Bill offers the best guarantee possible that Departments will address the needs of people with autism and that they will do so through a co-ordinated approach. There is a mechanism for Departments to be held to account. I am not aware of any Bill that goes into the type of detail that you suggest is needed to ensure the 100% delivery of services to meet each and every need.
815. The Chairperson: There could be a clause calling for a review of the effectiveness of the strategy in three years' time or some mechanism that would allow us to check what progress has been made. That is common.
816. Mr D Bradley: That is included in the Bill.
817. The Chairperson: Sorry. You are right, and it is to happen every seven years.
818. We now move into the territory of the rest of the Bill. We have considered the DDA, the strategy and the costs. Do members wish to raise any other points? Technically, our role is to go through the objections to the Bill clause by clause and question witnesses about them. I tried to dig out as many of those objections as I could, but I do not think that we have covered all of them.
819. I have to ask you a difficult question, Dominic. What is your reaction to the overwhelming decision to ditch the Scottish Bill by 109 votes to 5? It was an incredible, even overwhelming, majority, and it was not achieved through party Whips nor through a decision by the governing party. Clearly, the vast majority of MSPs took the decision that they were not happy to go down that road. Does Northern Ireland not have a lesson to learn from that?
820. Mr Bradley: If you do not mind, I will ask Arlene to respond to that question.
821. Mrs Cassidy: As members know, there is a Celtic Nations Autism Partnership, the Scottish element of which campaigned for a strategy. Therefore, our understanding is that a strategy is its preferred option. Within the Celtic Nations Autism Partnership, there is an understanding that certain jurisdictions do not need legislation to achieve joined-up working because their political structures are sufficient.
822. The Chairperson: That is an interesting point. Given that legislation is not required in Scotland, it is clear that government, through its own volition and without the big stick of legislation, can deliver the sort of joined-up approach that you want. Why can Northern Ireland not go down the non-legislative route?
823. Mrs Cassidy: I refer you to the original report by an Assembly researcher Vincent Gribbin, which considered a strategy for Northern Ireland versus legislation. The conclusion of that report was that Northern Ireland's particular governance structures require a legislative imperative to compel Departments to work together. Such an imperative is not needed in other jurisdictions. In Wales, for example, the equivalent of three of our Departments came together behind a strategy, and that was a Welsh Assembly decision. That is similar to what is happening through the process of the Bill. The Bill simply requires Departments to work together, which they did voluntarily in Wales, and as I hope that they will do in Scotland.
824. Mr D Bradley: Earlier, someone, and I am not sure whether it was the Chairperson or another member, said that he had questioned the Department of Health, Social Services and Public Safety about the extent of its knowledge of the Department of Education's work on autism. He discovered the Health Department's ignorance of what was happening in the Department of Education. If there was a sufficient degree of co-operation between Departments on the issue, there would be no need for a Bill. However, that level of co-operation is clearly not happening between the major Departments and the other Departments that need to be involved. That is why we need the Bill here in Northern Ireland. As Arlene said, that level of co-operation is available in Scotland. Unfortunately, it is not available here, and, perhaps, we adopt more of a silo approach. The Bill hopes to encourage Departments to break down that mentality.
825. The Chairperson: I asked that question of the Department this morning. It is a valid argument.
826. It is 6.10 pm. My next appointment is in Banbridge at 8.00 pm, and, therefore, I have to leave at about 7.00 pm.
827. Mr Callaghan: May I ask a quick question about the detail of a clause?
828. The Chairperson: Is your question on the miscellaneous end of the Bill?
829. Mr Callaghan: I did not get to ask a question on clause 3. Clause 3(2) states that the strategy:
"shall include the health care, educational and social needs of persons with autism."
830. Interestingly, the references in the presentations from the Department of Health, Social Services and Public Safety and the Department of Education almost invariably, with a couple of minor exceptions that were stimulated by members' questions, were always to each other, as opposed to other Departments. However, there are issues for umpteen Departments, including the Department for Employment and Learning, the Department for Social Development and the Department of Agriculture and Rural Development.
831. The word "social" is used in clause 3(2). However, the explanatory memorandum does not explain what it considers "social" to mean. As the promoter of the Bill, Dominic, what do you believe that it should encompass, and why did you not include words such as "training" or "housing"? If being more specific helped to stimulate a cross-silo mentality in the two big Departments, would you consider that?
832. Mr D Bradley: Are you asking why I used the word "social"?
833. Mr Callaghan: First, what do you mean by "social"? Secondly, why did you not specify, for example, training or housing? Would you think about being more specific by going beyond healthcare and education? I have listened to testimonies from different witnesses, and the legislation is almost viewed as a silo-busting Bill between the Health and Education Departments. That tends to reinforce the point that many people, although not everyone, regard the Bill as being about children, and that is particularly the case when education is mentioned. If training or housing needs were mentioned, that might broaden how the Bill is perceived.
834. The Chairperson: Do you have a question?
835. Mr Callaghan: I have put a few questions.
836. Mr D Bradley: Pól asked what I meant by "social", which I accept is a wide term. Perhaps he is right that a more specific definition might be required. The National Autistic Society, for example, suggested that we should, perhaps, have included a reference to employment. "Social" covers a vast area and could include, for example, the leisure and sports responsibilities of the Department of Culture, Arts and Leisure. There is also a need for supported housing to enable people with autism to live independently. We could, perhaps, give that further consideration. The problem is that we might end up with a fairly long, but still not exhaustive, list.
837. Mr Callaghan: With all due respect and deference to our mandarin class, some departmental officials might interpret "social" as referring to the Department for Social Development and, as a consequence, not take on any responsibility. Even a word such as "other" might help. If Dominic or the Committee were minded to submit amendments that refer to, for example, employment or training, other issues could be included.
838. Mr D Bradley: That is a very useful suggestion, and it is one that we will certainly consider.
839. The Chairperson: Dominic and Arlene, thank you very much. Once again, I apologise for keeping you waiting for so long to defend your Bill. As far as you are concerned, the pain is over until the Bill reaches the next stage, which will be when the Committee report goes to the House.
840. Mr D Bradley: May I ask a question before we finish? If we were to consider amendments other than those that we touched on today, would the Committee wish to be informed of them?
841. The Chairperson: Yes, unless the amendments are purely technical or grammatical. If they are substantive amendments, we need to know about them, because next Thursday is our last opportunity to come to a conclusion on the Bill.
842. Mr D Bradley: Does the Committee required the wording of those amendments or just an indication of what they might be?
843. The Chairperson: Yes, we definitely need the wording — you have a week.
844. Mr D Bradley: Chairperson and Committee members, thank you very much for the opportunity to present to the Committee. If there are no further questions, may we leave?
845. The Chairperson: Before you do, Mickey Brady wanted to make it clear that his leaving was not a walkout or a boycott. He would have stayed had he been able to, but he had to attend another function.
846. Mr D Bradley: I met him outside, and he apologised to us. Thank you.
20 January 2011
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Mickey Brady
Mr Pól Callaghan
Dr Kieran Deeny
Mr Alex Easton
Mr Sam Gardiner
Mr Paul Girvan
Mr John McCallister
Ms Sue Ramsey
Witnesses:
|
Mrs Dorothy Angus |
Department of Education |
847. The Chairperson (Mr Wells): We will hear from the representatives from the Department of Education (DE). Dorothy Angus is the director of access, inclusion and well-being; Debbie Gladwell is the head of the special educational policy advisory team; and Gillian Boyd is a DE official. Ladies, you are very welcome. The Department of Education has tabled a paper. Ladies, we would normally ask you to give a 10-minute opening address, which would be followed by between 45 minutes and an hour for questions. However, I suspect that the session will not be as long as that.
848. Mrs Dorothy Angus (Department of Education): Good morning, Chairman and members of the Committee, and thank you for the invitation. My short presentation will be on the educational framework in which an autism Act would operate. A briefing paper has been sent, and I hope that you have it. I have a short summary, if members would find it helpful, with some of the key points; it is to those that I will speak.
849. The education sector has a legislative framework for special educational needs under the Education (Northern Ireland) Order 1996 and the Special Educational Needs and Disability (Northern Ireland) Order 2005 (SENDO). More details of the provisions in the legislation are set out on pages 7 to 10 of your briefing paper, so I will not go into them other than to say that they are extensive and cover definitions, duties, education in special and mainstream schools, statements, appeals mechanisms, advice to parents etc.
850. The 1996 Order marks the start of a more contemporary approach, where special educational needs are mainstreamed and recognised as an integral part of education provision. It also marks the beginning of the inclusion agenda, as SENDO gave parents stronger rights to have their children educated in mainstream schools. Of course, there is more to the concept of inclusion than that: it means that all children should feel full and valued members of the school population.
851. The legislation is supported by clear, published, practical guidelines in the 'Code of Practice on the Identification and Assessment of Special Educational Needs'. That code is provided for in the legislation; it gives detailed guidance and is a key document for all those who deliver support to children with special needs in the education sector. There is a duty on education and library boards and on schools to have regard to the code, and in practice they all work to it.
852. Importantly, there is a statutory duty on education and library boards and on the boards of governors of schools to secure provision for a pupil's learning difficulty. Another important principle of our framework is that support is provided according to the individual needs of the child arising from a learning difficulty and not according to a specific condition or disability. That applies to children and young people with autism, support for whom is not dependent on their autism.
853. The definition of special needs in the legislation is broad. Section 3(1) of the 1996 Order states that:
"a child has 'special educational needs' if he has a learning difficulty which calls for special educational provision to be made for him."
854. "Learning difficulty" is defined as when a child has a significantly greater difficulty in learning than the majority of children of his or her age. In the accompanying guidance to schools on recording children with special needs, autistic spectrum disorder (ASD) is regarded as a special needs condition that relates to communication and interaction. In the briefing paper, we have given you case studies that outline the kind of support that is provided to children with autism. The intervention is matched to the individual needs of the child.
855. SENDO introduced for the first time disability discrimination laws for the whole of the education sector. Between 2002 and 2009, the prevalence of autism in schools, as recorded in the schools' census, increased by 243% from 1,158 pupils to almost 4,000. In 2002, the task group on autism highlighted an autistic spectrum wave rising through the school system. Therefore, the increase was not unexpected. It could represent something of a success in the education sector because the findings cover the period 2002 to 2009, which is after the task group report. It may reflect, to some extent, a greater response in education to the needs of autistic children, as more of them are recognised and recorded in the schools' census.
856. Much of the increase has been in mainstream schools, which may reflect the greater propensity of children with special educational needs to attend mainstream schools. However, some of it may be in the higher-functioning end of the autism spectrum. During the same period, the prevalence of special educational needs generally increased by 36·3% in the school population; it now stands at just over 63,000. That means that 20% of pupils have a special need.
857. Autism has been a priority for the Department since the report of the task group on autism in 2002. That report recommended areas for improvement and set an agenda for 10 years. Since the report was published, £9·3 million in addition to the normal spend on special educational needs has been expended to put in place measures to address ASD.
858. On page 13 of the briefing, you will find the measures that were put in place. I will highlight only one of those: the establishment of an inter-board autistic spectrum disorder advisory service. That service brought greater focus and cohesion to the support for children with autism, with multi-agency and multidisciplinary assessment services, common frameworks for assessment and training for parents and staff. The Education and Training Inspectorate reported very favourably on the service in 2009 and suggested some improvements around a regional service and a preschool support programme in tandem with the Health Service.
859. The inspectorate also recommended that a strategic policy be developed to map progress against recommendations in the 2002 task group report. That mapping exercise was undertaken in 2010, and work on developing a strategic framework and implementation plan is ongoing. The areas for improvement that have been identified include collaboration between the Department of Education and the Department of Health, Social Services and Public Safety (DHSSPS) to ensure continuity in policy and strategic approaches; further collaboration between the education and library boards and the health trusts to promote uniformity and cohesion in health and education provision; addressing the increasing demand on resources to ensure more equitable and effective provision; and shaping policy development through local and internationally based research.
860. Finally, in parallel and led by my colleague Gillian Boyd, we are undertaking a capacity building programme for the school workforce, particularly in mainstream schools, to equip it better to support children with special needs, including autism. As well as direct training, that includes a resource pack for schools, which will be available electronically as well as in hard copy. People from the health sector have worked with us very closely in the development of that programme.
861. The Chairperson: Thank you for your presentation, and thank you for being spot on time. It may be stating the obvious, but we are here not so much to hear about the excellent work that is being carried out by the Department of Education in this field as to get the Department's comments on the private Member's Bill that is sponsored by Dominic Bradley.
862. In the Minister's letter and your presentation, I notice that, although you emphasised the ongoing work that you are doing, you have not actually stated your opinion, as a Department, on the Bill, on either the amendment to the Disability Discrimination Act (DDA) or the proposal for an interdepartmental strategy, which would encompass many Departments and would include your Department as a major player. In her letter, the Minister said that she supported in principle at Executive level the concept of the Bill and that she has sought views in the Department. Is that right?
863. Ms Debbie Gladwell (Department of Education): We have started a pre-consultation exercise on our autism strategy. We intend to go out to consultation as soon as we possibly can once that pre-consultation has finished. I have written to the Education Committee to say that we will be doing that.
864. The Chairperson: Does that mean that you are not in a position to say what your views on the Bill are?
865. Mrs Angus: In her letter, the Minister says that she supports the principle of the Bill and that there is a need to consider the impact of the Bill on the current legislative framework. We cannot divorce the Bill from the current legislative framework, which is why I have set it out for you this morning. The particular issues that the Minister feels need to be looked at are the Bill's potential to create a hierarchy of special educational needs, to create an imbalance in the budget for all special educational needs and to impose unnecessary bureaucracy. You mentioned the consultation point. Those are the issues that the Minister would like us to follow through on to a greater extent.
866. The Chairperson: If the Bill, as it is presently drafted, became law, what would the implications be? How would the redefinition of the DDA and the overall planning strategy impact on the Department of Education?
867. Mrs Angus: As I have outlined, under the current legislative framework, the support is provided in relation to the specific learning difficulty that the child has, not on their having autism as such. The priority for us is not the condition; it is whatever difficulties the child has. In that sense, our legislative framework would be able to continue in that way because it is not impacted by the precise definition.
868. The Chairperson: Are you basically saying that, as things stand, the Department could continue to develop that work and so the Bill would not make any substantive difference to what you are doing already?
869. Mrs Angus: No. It would not impact in definitions because it does not depend on a DDA definition or the condition.
870. Ms Gladwell: Dorothy has already described the special educational needs (SEN) framework. It is robust, and I go back to it for a reason. The 1996 Order brought in inclusion. Then, in 2005, SENDO brought in two main aspects that the Committee will want to consider. The first part was the SEN aspect of provision and strengthening parents' right to inclusion. The Committee, in the evidence that it is considering today, must look at the Autism Bill within the context of that framework.
871. The second part is in relation to SENDO and the disability discrimination aspects. It strengthened the rights of children to be educated in ordinary schools, and it brings about responsibilities as it links the legislation to the Disability Discrimination Act and the definition that is described in it. Therefore, our SEN framework links to the current disability discrimination legislation. It places a lot of emphasis on education and library boards and on schools to ensure that they do not discriminate against pupils with a disability. One of the main thrusts of SENDO is that it links to the current Disability Discrimination Act and brings that legislation right in to the school. It places very strong duties on education and library boards and on schools to ensure that they make adjustments so that pupils who have a disability are not put at a substantial disadvantage compared with pupils who do not have a disability.
872. It also places a very strong duty on them to ensure that the pupils have an equal right and that there is nothing that prohibits children with a disability from accessing education and even the premises and the curriculum. Therefore, it makes it illegal for schools and education and library boards to discriminate against disabled children, for example, in their admission arrangements, in the education and in any associated services that are provided by the schools for its pupils. That even relates to pupil exclusion from school.
873. If that is abused in any way — legislation, no matter who it applies to, does not always go right and can be abused — there is a right of appeal. The SENDO legislation — this is why I keep going back to the framework that we have — expanded the old SEN tribunal to become a Special Educational Needs and Disability Tribunal (SENDIST) so that it was able to hear disability discrimination cases. It is important to understand where our legislation sits as regards disability discrimination and, if there are changes, how that may change that type of legislation.
874. The Chairperson: We are playing devil's advocate. We are being told that the Bill will lead to a radical change in how we treat autistic children in terms of medical provision, social services, education and so on. You are basically saying that, because you take the view that it is not the label but the needs of the child, you are addressing that already. You do not see any radical change.
875. If there was a cross-cutting Executive strategy that encompassed all Departments and took in the needs of those with autism from cradle to grave, would that lead to a radical change in how we treat and deal with those who have autism?
876. Ms Gladwell: For the past year, in developing its strategy, the Department of Education has been working closely at every level with its counterparts in the Health Department, from the Department itself to the Regional Autistic Spectrum Disorder Network (RASDN) and the Health and Social Care Board. The opposite is also true: education and library boards and the Department have been interlinking throughout all that work. That work has developed the strength of strategies. For example, in the mapping exercise that the Department has been undertaking over the past year, we have had representation and input right through to the development of areas for improvement, including identifying and building on the strengths that exist.
877. Strengths exist already in interdepartmental, inter-agency working. We have identified areas for improvement on the basis of advice from the Education and Training Inspectorate as well as that of colleagues from the Health Department. We will ensure that whatever strategy comes out of the Department of Education links into the health strategy.
878. The Health Department's strategy has identified five areas for improvement and has looked at the four key areas under its care pathway. That involves looking at early assessment, which the Department of Education wants to do for the preschool package, so linkages exist there. It then covers diagnosis as well as the interventions that will be put in place. Again, that is relevant to educational interventions. The strategy will cover the transition arrangements and will strengthen the linkages between education and library boards' ASD and transition services and those of the health trusts. Therefore, a cross-cutting, cradle-to-grave strategy that involves the education of children is already being worked on.
879. The Chairperson: Would it be more effective if the Bill compelled Departments to work together in a single strategy rather than each Department going its own way and co-operating only if it deemed it appropriate?
880. Mrs Angus: It is difficult from this perspective to know whether that would be the case because so much work is going on to which we are all committed. We look at special educational needs across the board, so creating an environment in which there is a strategy for one particular special educational need that is set out differently from that for all the other special educational needs might create difficulties and a hierarchy. We are developing our strategy with our colleagues in the Health Department in the broader framework of special educational needs.
881. Mr McCallister: I was going to ask Dorothy about that hierarchy. If the Bill becomes law, is there a danger that the condition becomes more important than the need? Am I overemphasising the risk? In fairness to the sponsor of the Bill, I do not think that that would be an intended consequence. However, is that your understanding of what would happen if the Bill were enacted? Like the Chairperson, I am not getting a clear steer on whether the Bill will be an advantage to your Department or whether you are saying that, like the Health Department, you have all the tools that you need.
882. Mrs Angus: We feel that a strong legislative framework already exists that does not depend on a condition. Children with conditions are listed under various headings; that is how they are recorded in the schools' census. However, the important thing is that that is not how the support is provided. It is difficult to say whether highlighting the condition, as opposed to the need, could ultimately cause a problem. If we maintain our legislative framework, we will continue to give support in the education sector according to the need. That is probably the only way that it could work. We have to concentrate on the learning difficulty that may be related to the condition, because that is what exhibits in school.
883. Mr McCallister: If the Bill is passed, will you have two competing pieces of legislation? If so, which one will take priority? That will be the problem. We are all open to your guidance on that; this evidence session is about hearing which one you think will take priority or how you will square that circle.
884. Mrs Angus: We certainly feel that it is an area on which we need a clearer understanding, and we are taking advice on how much it might impact on our ability to consider the need or to provide equity of support across the range of special educational needs. We would not want to move away from a focus on all of the needs that we consider to have equality in our system. We need to do a little bit more work on that to be sure that we understand what such a situation might mean.
885. Mr McCallister: It would be useful for the Committee to have an answer to that issue. We could really do with having that, bearing in mind that the Bill is progressing at a fairly rapid pace and could be back before the Assembly for its Consideration Stage in February. We do not have a lot of time to act.
886. I am encouraged by your Department's response and its collaboration with the Health Department in early diagnosis, treatment or support. What happens if the Bill compels you to do a strategy and the Departments cannot agree on that strategy? The obvious example of that is the Middletown Centre for Autism. Your Department is committed to that project, and the Minister mentions it in her opening letter. Obviously, the Health Department has a different view on that. Where would the Bill leave you on such issues where the two Departments, or, as the Chairperson said, as many as seven or eight Departments, are trying to form a strategy and get a combined way forward?
887. Mrs Angus: That might depend on how any strategy is funded. If each Department continued to fund and to have a degree of control over its own strategy, there would presumably be more scope for Departments to have their own priorities in the strategy for how they address autism. If there was one pot of funding, that is where the tensions would start to arise, because, as you say, there are things that we are doing specifically and there are other things on which we are working very closely with other Departments to deliver on the ground. For instance, the collaboration between people in the health and education sectors is quite close, and I suspect that there would be quite a lot of agreement on how that would be dealt with. However, there are areas for which we would have to give very clear consideration to our particular priorities.
888. Mrs O'Neill: I will pick up on the last point that John made. If Departments cannot agree, surely that is the point of our legislating for a strategy in the first place. Departments might work together on many levels, but there are many instances where they do not. We are all very realistic around this table, and I am quite sure that everybody knows that, unless it has a lead responsibility, quite often a Department will sit back and let someone else take responsibility. We want to legislate for a strategy to address that very point, which is why we need to push forward with it.
889. The Department of Education has already started the work on the autism strategy. If this legislation is passed, there is no reason why that work cannot fit in and carry on. In some senses, the Department of Education is ahead of the legislation, because the work is already happening. That is a point that I wanted to make.
890. Dorothy, you said that a strong legislative framework is already in place. Your point was that amending the Disability Discrimination Act would have no impact on the service that is provided to children in schools. So, there is no harm. It would not have any direct or negative impact on services that are already provided.
891. Mrs Angus: It appears that that would not impact on the way that we provide services to children, because, as I have said, we provide according to need. The impact that we are looking at, which we have already covered, is the hierarchical one. We need to understand that more clearly. However, considering that the legislation is framed in terms of a strategy, I do not think that there would be any impact on the way that children are provided with services. However, I do not know how the courts might read it in the future.
892. Mrs O'Neill: When do you think that you will be in a position to comment more on the impact of the Bill on, for example, SENDO? Debbie, you picked up on that point.
893. Ms Gladwell: We would have to have received advice from a few areas on that. We are currently seeking that advice, so we will comment more as soon as possible.
894. Mrs O'Neill: Given our timetable for getting through our scrutiny of the Bill, will you try to hurry that along and to share your views with the Committee as soon as possible? Even if you cannot come before us again, you could send your views to us in written form.
895. Ms Gladwell: Yes, we will.
896. Mr Easton: I agree with the Deputy Chairperson: if passed, the Bill will not do any harm. It is good to know that you agree with that.
897. Your strategy with the Health Department is good in so far as it goes, but there is no joined-up strategy with other Departments on vital issues. For example, I am dealing with a case in which the parents of a child with autism are applying for disability living allowance (DLA). Many parents of autistic children receive that benefit for their children, but this child has been turned down. The DLA application was not turned down because the parents did not have the medical evidence from their GP and other health professionals; it was because of the report from the school, which put the child down as being hyperactive and naughty. We have to go through an appeal, and I believe that the decision will be successfully overturned.
898. That is an example of a lack of a joined-up approach between the Department for Social Development, the Health Department and the Department of Education. If the Bill is passed, can you see a joined-up approach emerging as a result? Such an approach is essential, because there are some children missing out. Do you see a joined-up approach between all Departments being a good thing?
899. Ms Gladwell: As regards advice from schools, I am not clear how the strategy could influence advice from schools in the way that you described. I am not familiar with the circumstances of the case that you mentioned, so I cannot comment on it.
900. Mr Easton: There are teaching staff who have failed to recognise, despite the medical evidence, that a child has autism. Consequently, they have failed the child and the family. Obviously, there is a lack of understanding about autism and, in certain elements of the education sector, a lack of awareness training. Your strategy will probably address some of those issues, but there are failings. The Bill is vital to ensure that there is a joined-up approach between all Departments to help to deliver the best for a child, not just in health and education but through access to benefits that they are entitled to.
901. Ms Gladwell: The training aspect of any strategy is vitally important. The Department of Education is currently undertaking a capacity building exercise around all SENs in the classroom, which includes training in autism. Gillian might want to comment on some of her work.
902. Ms Gillian Boyd (Department of Education): As a former principal of two special schools, I have had to fill in many of those forms. Schools are not asked about the diagnosis or the condition in those forms; they are asked about how the behaviour presents in the experience of the school. The school has to truthfully reflect how the child behaves instead of concentrating on the diagnosis. So, I cannot see how any changes would impact on the advice that schools give in those forms.
903. Mr Easton: Better training would make teachers more aware of the condition, which means that, when families who are applying for DLA need their support, there would be a better understanding and families would not be losing out. It is a failure on the part of the Department of Education that that has not happened. That might be addressed in your review, but I do not know, because I am not totally au fait with your strategy. Obviously, your strategy is a good thing, but the joined-up approach is not quite working yet. You may need to think about that a wee bit.
904. Ms Boyd: I am on secondment to the Department of Education and work for the Education and Training Inspectorate as an inspector for special education. As part of that role over the past five or six years, I have been looking at SEN in mainstream and special schools. I can honestly say that I have not come across any school that is not aware of ASD. Expertise on ASD varies from outstanding to good and satisfactory. I can truly say that in the many schools that I have inspected, I have not seen a lack of awareness.
905. We have ASD training teams in each board; we have the Middletown training and advice centre for the more complex youngsters; and we have sent out a training tool to all schools for all staff to access whenever they wish. We have a team putting together strategies that every classroom teacher, every classroom assistant and every principal will be able to access. Those will be written by outstanding practitioners in the field; classroom teachers, principals and advisers who are working to disseminate their outstanding practice. When we looked at a Northern Ireland-wide survey of ASD, we found that practice ranged from good to outstanding. There is always room for improvement; we would like to see every school become an outstanding school.
906. Mr Easton: As part of your strategy, you are providing access to measures that make everybody aware of autism.
907. Ms Boyd: No. We are providing access to measures that help school staff become outstanding in their practice.
908. Mr Easton: Will that be mandatory? Will staff know about that?
909. Ms Boyd: They will certainly all know about it.
910. Mr Easton: You might want to consider Millisle Primary School, because the staff there obviously do not know much about autism at the moment. You might want to take that back.
911. Mr Gardiner: Thank you for your presentation. Will the Bill give you additional powers to look after children with autism? We want the best for those children.
912. Mrs Angus: The Bill requires that the Departments devise a strategy. We are already devising a strategy in conjunction with our health colleagues. I am not sure that the Bill gives us any further powers.
913. Mr Gardiner: So, you have the power at the moment without the Bill.
914. Mrs Angus: We have the power to provide for the children.
915. Mr Gardiner: Will the Bill allow you to implement more than you can do with the powers that you have at the moment?
916. The Chairperson: That is an important point. Is there anything that you would like to do but cannot because you are constrained by legislation in the education sector?
917. Mrs Angus: No.
918. Mr Gardiner: There is nothing more that you can offer.
919. Mrs Angus: There is nothing that legislation constrains us from providing.
920. Ms S Ramsey: The fundamental issue is that there are a lot of laws out there. Sometimes, Departments do not carry them through because of the financial aspect. The Bill will make it a legal duty to act rather than a statutory duty. That is the key point.
921. The Chairperson: Is there anything that you are not doing at the moment that you feel that you would be forced to do by the Bill?
922. Mrs Angus: I come back to the point about the hierarchy. Would we be forced to give priority to children with autism over children with moderate learning difficulties, severe learning difficulties, dyslexia and all the other range of special educational needs?
923. The Chairperson: Presumably, with a finite budget, if autistic children were given priority, it would be to the detriment of those other children.
924. Mrs Angus: We are concerned about that. That is the issue that we have already mentioned; we need to understand better whether the Bill would put us in that position. I do not think that there is anything that the Bill helps us to provide for children with autism that we are not able to provide with the powers that we have at the moment.
925. Mr Easton: Chairperson, your question is very unfair. There is nothing in the Bill to say that autism will get priority over anything else. To say otherwise is very misleading. I do not agree with that analysis, and there is no proof for it. I want to put on record that there is nothing in the Bill to suggest that autism will be given priority over any other disability.
926. Mrs Angus: I have not suggested that either. I said that we need to understand better whether that could be the result of the Bill.
927. Mr Callaghan: I very much concur with what Alex has said. It is very important that we do not overhype the potential of the Bill. That could be a downside from the perspective of some people, but it also does away with some of the objections that are being raised to the Bill.
928. I want to touch on the degree of co-operation between Departments. In some of the evidence that has been submitted, every Department and agency has received some criticism for what they are doing or are not doing. I cannot speak for other members of the Committee, but it seems to me, from a lot of the evidence that we have received from parents, carers and representatives of some of the autistic spectrum disorder groups, that people are not properly co-operating and co-ordinating. That seems to be the problem. It is not necessarily that there is a deficiency in what they are doing. What is the Department's view on the potential for better co-operation between it and its agencies — my definition of which includes schools — over and above what exists?
929. We are getting a wee bit confused in this session about the importance of definition in bringing about a step-change in services. The definition, to some extent, stands on its own in the DDA-related clause. Aside from the first clause, the Bill's clauses deal with the strategy, and they are not predicated on the definition per se. I am just interested in your view on there being better co-operation and co-ordination.
930. Let me put it like this: everything that the representatives from the Department of Education have said here today, just like everything that the representatives from the Health Department and other statutory bodies might have said to us before, has been — this is not necessarily a criticism, but it is certainly a reflection of the governmental approach — about how the Department responds when it encounters those issues. In contrast, the Bill is trying to change the paradigm so that we can say how a family is responded to by the system in its entirety, regardless of what part of the system it is dealing with, be that a school or something else.
931. The Chairperson: Is there a question coming?
932. Mr Callaghan: What do you think of that? [Laughter.]
933. Mrs Angus: We agree with you — the end result of whatever we do ought to be the support that we provide for the child and that support ought to be joined-up. I entirely agree with you. In the mapping exercise that we did for our strategy, some of the areas for improvement that we uncovered related to collaboration at all levels: for example, collaboration between the Departments, which we have been making efforts to improve — I see some of my health colleagues here — and the way in which the professionals on the ground work to support the children.
934. So, there is scope for improvement, and it is good that we do everything that we can to ensure that that happens. Debbie has been working on the strategy and has been working very closely with our health colleagues at the policy and delivery levels to try to do that.
935. Ms Gladwell: I will tease that out a wee bit more. There has always been collaborative working between the two sectors, but there has also always been room for improvement in that. We have evidence that collaboration has already been established. We have issued documents that have identified standards for collaborative working.
936. On the autism strategy specifically, we have been working very closely with our health colleagues. Our work has been so closely linked that we have almost been speaking with one voice. Our health colleagues have been working very closely with my education groups to determine where the gaps are and to identify the areas for development. We have discussed whether those gaps are at a departmental level and have agreed that we should link the education strategy strongly with the health strategy and have a joint statement of some sort to strengthen both strategies by bringing them closer together.
937. In addition, we have RASDN, which is a health-related network that has representatives from education and library boards sitting on its board. I also have a seat on that board. However, education and library boards and trusts must work together more closely and be much more collaborative. The strategy seeks to identify collaboration as an area for improvement and to have specific actions in place to formalise that arrangement. There will be full, 360 degree reporting back, through the implementation plan and a joint implementation group, so that we can ensure that that is happening.
938. So, collaborative working is a good thing. It has to continue to be improved on, and we have to continue to ensure that we put those actions in place. That will be done through the draft strategy and the implementation plan. It will report back through the existing structures, and the two Departments will have a monitoring role to ensure that there is collaborative working. There are examples of good practice. We have evidence of collaborative working between the two Departments in certain areas, and we want to strengthen that even further.
939. Mrs Angus: What Mr Callaghan said is right: we need to recognise that, at the end of the day, parents do not care whether the support comes from the education sector or the health sector; they just want the support for their children.
940. Mr Callaghan: Although what you are saying is positive to an extent, it is only fair to say that it does not tally with everything that we have heard about user experience.
941. One thing that I found very interesting in what the Health Department provided us with this week was that there was not really any reference to any Department other than itself and the Education Department on the issue of collaborative working. The Bill's provisions are not restricted to childhood. In the transition phase for people aged 18 or 19 years, is there much scope for improvement in relationships with other Departments and their agencies? The Department for Social Development (DSD) and the Department for Employment and Learning (DEL) come to mind, in particular. The Bill is not aimed at just the Department of Education and the Health Department.
942. Mrs Angus: We have had a couple of exercises on that. The Department of Education led an exercise a few years ago on transitions, when there was an action plan and so on. Presently, as part of the ministerial group on children and young people, I chair a group that looks specifically at transitions. That group has on its membership not just the health partnership, which, as you said, has been mentioned quite a lot today, but DSD, because it looks at housing. There are also representatives from the Department of Justice on the group, because too many young people with special educational needs end up in the justice system because they have not done well in education. Debbie, remind me of the other Departments represented on the group.
943. Ms Gladwell: There is the Department for Employment and Learning.
944. Mrs Angus: That Department is represented because young people in their transition years move into further education when they leave school.
945. Mr Callaghan: Some do not.
946. Mrs Angus: Yes. We recognise that all those Departments have to work together to ensure that, when young people move on from school, they move into something meaningful. A lot of them move on from special schools, where they have been given a lot of stimulation that meets their needs. Perhaps, the broader system has not been able to meet those needs so far. We presented our action plan on that to Ministers, it was approved, and we are working on moving it forward.
947. Mr Callaghan: So, a statutory duty to co-operate would not necessarily run against those efforts.
948. Mrs Angus: No.
949. Dr Deeny: I apologise for missing your presentation; it took a lot longer for me to get down this morning than I had anticipated.
950. I want to ask about an issue that you may have covered. It was touched on by Mr Easton. There has been mention of a hierarchy of disabilities and a concern about disabilities being prioritised. There are a lot of teachers in my family; my wife and my brothers and sisters are teachers. What are the views of principals and senior teachers?
951. In my practice, we have people with all sorts of disabilities, including children with muscular dystrophy and cerebral palsy. Are some of the senior teaching professionals concerned that the Bill would prioritise disabilities? For example, autistic spectrum disorder has a spectrum, and I can think of some people who are severely autistic. I like the fact that you are talking about the individual needs that arise from a learning difficulty. Some people are at the milder end of the spectrum. Is there concern that someone at the milder end of the spectrum will receive the support that they need and that someone with another disability, such as cerebral palsy, will not? I would not like to see that happening. Is that a concern among senior teachers? Do they know about the Bill?
952. Who assesses the individual needs of a schoolchild? Is it the principal? Severely autistic children need a lot of support, whereas, at the other end of the spectrum, children with Asperger's syndrome who are quite intelligent may not need much support. Who makes that call? Do you know of any concern among senior and experienced teachers about the Bill leading to a prioritisation of disabilities?
953. Mrs Angus: I will answer the second part of your question first, because it may lead to an answer for the first part.
954. The determination on the support that a child needs is made according to the code of practice that I referred to in the presentation. That code of practice has five stages, some of which are school-based and others, for children with more challenging needs, are based in the education and library boards. The fifth stage is where a child is statemented, because he or she has the most challenging of special educational needs. Therefore, sometimes the school will be able to determine what is needed and will be able to put that intervention in place. However, in some cases, an educational psychologist will be needed to consider the child, who will be taken through all five stages of the code of practice. Autistic children will go through that process as well. Is there anything to add to that, Debbie?
955. Ms Gladwell: The teacher makes an assessment in the classroom based on the behaviour that the child presents. The stages of the code of practice apply at that point, and the child is placed on the SEN register.
956. Mrs Angus: Some children are on the SEN register, and some are statemented. I said earlier that 20% of children in our schools have a special educational need, but they will not all be at the statemented stage.
957. That is the context in which to answer the first part of your question, Dr Deeny, because that is the framework within which schools are used to operating. Schools are used to treating special educational needs by looking at the learning need of the child, not the condition that the child has. Schools look at the specific learning need and what support they need to put in place.
958. In those terms, we have heard, through the teachers' unions, some concern about the Bill. That goes back to the question of hierarchy, which is one of the reasons why we are seeking to understand that better. That is also one of the reasons why the Minister has asked us to look at the particulars of the Bill. We have made it very clear that the Minister supports the principle behind the Bill, but she has asked us to better understand the hierarchy issue, because we are hearing concern expressed about it, although not a huge amount.
959. Dr Deeny: I presume that principals and senior teachers have looked at the Bill, are aware of it and are interested in it.
960. Mrs Angus: They do have awareness of it, although I cannot say to what extent. Certainly, the unions have been looking at the Bill, and they normally represent the voice of the teachers.
961. The Chairperson: I predicted that this would be a short session, but it turned out to be much longer, which is an indication of the content of what you told us. I should have declared an interest, because my mother, my wife and my two daughters are all teachers. That is not in the Register of Members' Interests, and this is the first interface that I have had with the Department of Education. This session has been very useful and has helped the debate considerably. Thank you.
962. Ms S Ramsey: Is that what Stephen Nolan calls nepotism, or does it only apply to politicians?
963. The Chairperson: I do not know what it is, but I think that it needs to be declared in this context.
964. Mrs Angus: Thank you for the opportunity to give evidence.
20 January 2011
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Mickey Brady
Mr Pól Callaghan
Dr Kieran Deeny
Mr Alex Easton
Mr Sam Gardiner
Mr Paul Girvan
Mr John McCallister
Witnesses:
|
Mr Charles Bamford |
Department of Health, Social Services and Public Safety |
965. The Chairperson (Mr Wells): We will now receive evidence from witnesses from the Department of Health, Social Services and Public Safety. I welcome Dr Maura Briscoe, who has been before us many times and who is the director of the mental health and disability policy directorate; Peter Deazley, who is also from the mental health and disability policy directorate; Charles Bamford — there is an obvious question, but I will ask it later on — who is a social services officer; and Dr Ian McMaster, who is a medical officer. You are all very welcome.
966. You have given evidence to us before on this important private Member's Bill. You have had the benefit of hearing the evidence from various organisations, particularly the charity groups, and you sat in on the Department of Education's evidence session this morning. As normal, feel free to give us a 10-minute introduction. I am sure that there will be many questions from members for you to answer.
967. Dr Maura Briscoe (Department of Health, Social Services and Public Safety): Good afternoon, everyone. Thank you for giving us the opportunity to come back. We look forward to having a fruitful discussion. Given the time constraints, rather than rehearsing the debate that we had previously, I propose to concentrate mainly on the clauses of the Bill. Therefore, what we say this morning represents the Department's view, which has been informed by legal advice.
968. The Department does not believe that it needs legislation to drive forward service change. Indeed, from our perspective, the legislation has the potential to cause disruption to current policy action and implementation.
969. Clause 1 would amend the Disability Discrimination Act (DDA) 1995. The Office of the First Minister and deputy First Minister (OFMDFM) is responsible for anti-discrimination legislation, and you may wish to consider whether to seek its views on the Bill. It remains our view that autism is covered by the DDA, as evidenced in practice by case law. Non-specific changes may have far-reaching consequences as well as potential costs that were not intended by the sponsor of the Bill.
970. Serious and specific in-depth consideration should be given by the Committee to the proposed changes to the DDA. I heard only the end of the previous evidence session, but we noted previous discussions in the Assembly and elsewhere about the linkage between the DDA and access to social security benefits. The proposed changes to the DDA will not improve access to social security benefits. The Department for Social Development takes the lead in that field, and you may wish to seek direct advice from it.
971. Clauses 2 and 3 relate largely to the development and content of a strategy. The objective of those clauses is not clear. If, for example, the objective is to protect the right of individuals to have their needs met, it could not be achieved without additional resources. That is the case not just for children but, as was said earlier, for adults and carers. However, it has been said that no significant costs are attached to the Bill.
972. On the other hand, if the objective of the Bill is to produce another strategy, the strategy itself will not necessarily improve front-line services. As a general principle, most legislation is underpinned by sound policy rationale. From the Department's perspective, this piece of legislation is not underpinned by sound policy. We already have an autism strategy, an infrastructure in place and resources that are attributable to autism.
973. The Committee will have received our paper, which notes that the Autism (Scotland) Bill was defeated at Stage 1 by 109 votes to five votes. It is worth noting that one of the reasons for that was that the Committee that was responsible for scrutinising the Bill was not convinced that legislation that is specific to autism would necessarily improve autism services. In addition, and perhaps more importantly for us, it was recognised that such an approach could have created a perception of "two-tierism", whereby some disabilities are deemed more worthy than others. That has resonance for us when it comes to compliance with the European Convention on Human Rights, particularly articles 14 and 8. For example, does someone with autism have more rights than an individual with an equally disabling or a more disabling condition?
974. Perhaps what underpinned the Scottish approach was the perception that people with a certain condition, in this case, autism, would benefit from the legislation while people with other disabilities would not.
975. Therefore, we ask the Committee to consider the competence of the Assembly to legislate for the matters that are addressed by clauses 2 and 3. I am not saying that they would be, but if those provisions were challenged under the European Convention on Human Rights, what would be the defence?
976. The human rights of all people with disabilities are important to us, but so too are the budgetary constraints of the environment in which we all have to live. I note that Minister Wilson wrote to the Committee this week, and he recognised that there is a financial cost to the Bill.
977. I will now turn to the costs of the Bill. The strategy has not been costed. As I said, one would first need to be clear about the objective of the Bill. Assuming that the strategy would have content, it would generate additional cost. In addition, it is noteworthy that clause 3 refers to training civil servants who deal directly with the public. As members will see in our paper, we estimate the cost of that to be £1·8 million. One could argue that additional resources would have to be found to pay for that, and that such resources would be better targeted at front-line services.
978. A public awareness campaign is also referred to in the Bill, which would not be without cost. In our paper, we have provided the low-end and the high-end costs. The low-end cost, which assumes that existing campaign material would be built on, is approximately £25,000. However, if there were a media campaign to raise public awareness that involved, for example, TV and Adshels, the cost could be more than £200,000. Therefore, there is a cost attached to the Bill.
979. I do not propose to address clause 4, which is about the definition of autism. We had a long discussion about that at a previous meeting. Our view remains the same: it is not in anyone's interests to define autism in legislation. That is because research on, and experience of, autism could potentially change, particularly as it is a spectrum disorder.
980. The Department's view is that the Bill would create bureaucracy and would not necessarily improve front-line service provision. It may be disruptive to our current autism action plan and the infrastructure that we have in place to deliver on that. We do not want to see any additional resources being directed away from front-line services. The Committee needs to give serious consideration to the potential unintended impact of clause 1 and the legislative competence of the Assembly on the provisions that I identified in clauses 2 and 3.
981. The Chairperson: Thank you, Dr Briscoe. To try to give some coherence to the questioning, we will start, as we did previously, with questions on clause 1, which seeks to amend the DDA. We will deal with any questions that members have on that first. We will then move on to questions on the strategy and co-operation between Departments. After that, members can ask questions on any other issues.
982. Clause 1 seeks to amend the DDA by inserting, ", social (including communication)". What do you see as the potential risk of that? To many in the Committee, that seemed to simply plug a loophole for children who fell between two stools. Some have physical needs, some have mental needs and some have neither but have real problems with social interaction and communication with their fellows. Where is the danger in what seems like such an obvious measure?
983. Dr Briscoe: The Department believes that autism is covered by the current DDA, which is evidenced by case law, and I am happy to talk about case law if you want me to. The Office of the First Minister and deputy First Minister guidance on the existing DDA clearly states that autism is covered. There are a number of examples in that guidance that are covered.
984. On the one hand, autism is covered in the DDA, and there is case law to support that, so why would you want to change it? Secondly, terms such as "social (including communication)" and "forming social relationships" are very non-specific. What do they mean? They do not mean anything specific to autism but are generic terms. What would such changes mean for the whole of society? What about the special adjustments that may have to be made by employers and so on?
985. The Chairperson: We are getting some research information later this afternoon on that specific issue. It is something that the Committee will have to look at.
986. Dr Deeny: I heard somebody on the radio this morning talking about people who have speech impediments. Those people have communication problems. Are you saying that including "social (including communication)" will mean that it will apply to people other than those who have autistic spectrum disorder (ASD)? There are people out there who have communication difficulties who are not autistic.
987. Dr Briscoe: The definition of disability and the impairment that arises from disability is specific in the DDA. There are a number of capacities included in that, including speech. Therefore, people with a disability that involves speech or communication difficulties that affect their day-to-day activities are covered by the DDA.
988. I draw your attention to case law. There is case law that involves a primary school and the behaviour of a child with attention deficit disorder. I came in at the end of the previous evidence session when Alex Easton was talking about similar case. The National Autistic Society joined the case, because, rather than the child's condition, the fundamental issue was whether the reasons for the child's disruptiveness in school were covered in the DDA. The case law went through due process, and it was found to be covered.
989. Another case involved a secondary school. Again, it was about behavioural issues, and involved a child with autism. That case went through the system, and the judge was very clear that the child's circumstances and autism were covered by the DDA. I am happy to quote that case law, if you let me.
990. The Chairperson: It would be helpful to have the reference so that we could have a look at it.
991. Dr Briscoe: I will give you the reference. The first case that I referred to took place in 2009, the reference is EWHC 1842 and the judgement was made by Justice Lloyd Jones. The second took place in 2003, its reference is EWHC 3045 (Admin) and Justice Silber made the judgement. Justice Silber said:
"The Act makes it unlawful to discriminate against a person who has a disability which for the purposes of the Act means that 'he has a physical or mental impairment which has a substantial long-term adverse effect on his ability to carry out normal day-to-day activities'': section 1(1). It is common ground that IC has a disability for the purpose of the Act."
992. The Chairperson: Basically, you are saying that the case law shows that autistic children and adults are covered by the DDA.
993. Dr Briscoe: Yes. [Interruption.]
994. The Chairperson: Order. Only members of the Committee are to ask questions, please.
995. Is there a fear that, as others said, the inclusion of the term "social (including communication)" could weaken the definition of "mental" and "physical"?
996. Dr Briscoe: As I said, the text of the DDA relates to the schedules, which, in turn, relate to capacities, and those are about the impacts of impairments on day-to-day activity. This legislation would add "social (including communication)" and "forming social relationships" to the list of capacities. A person needs only one thing from that list to impact on their day-to-day activities on a long-term basis to receive additional protections under discrimination law. The inclusion of the non-specific terms of "social" and "forming social relationships" would potentially widen what was intended by the DDA. It could also widen what was intended by the proposer of the Bill. The proposer of the Bill was interested in autism, but many people with conditions of varying severity also have difficulties in forming social relationships. Indeed, there are many people who do not fall into a clinical category but who have difficulty in communicating socially and in forming social relationships. Therefore, it could be argued that amending the DDA will dilute the mental and physical impairment side.
997. Mrs O'Neill: You said that the Bill could be subject to challenge under the European Convention on Human Rights.
998. Dr Briscoe: No, I did not say that.
999. Mrs O'Neill: It is in your paper.
1000. Dr Briscoe: I said that clauses 2 and 3 of the Bill might be subject to challenge. I was not talking about the amendment to the DDA clause.
1001. Mrs O'Neill: Are you aware that, in its paper to the Committee, the Northern Ireland Human Rights Commission stated that it believes that there will be no adverse impact from amending the Disability Discrimination Act?
1002. Dr Briscoe: I am not talking about the Disability Discrimination Act; I am talking about clauses 2 and 3.
1003. Mrs O'Neill: Your paper states:
"It is also of note that the proposed changes to the DDA, in our view, will not have the desired effect of increasing access to Social Security Benefits".
1004. Dr Briscoe: Indeed.
1005. Mrs O'Neill: What was the basis for that assessment?
1006. Dr Briscoe: Although I recognise that there is an interrelationship between the DDA and some aspects of benefits, such as the blue badge, the issue is how an individual meets the criteria for receiving, for example, disability living allowance. Therefore it is the impact of the disability and not necessarily the condition itself that has to be adjudicated. The Committee should take evidence from the Department for Social Development on the issue. In our view, it is the underlying need that arises from the disability rather than the condition itself that must be considered. That need would have to meet the criteria for access to certain benefits.
1007. Mrs O'Neill: With respect, Maura, that is how it should work; however, the reality is different. The Committee has heard evidence, and I have seen a tribunal decision, that autism is nowhere included in the Disability Discrimination Act.
1008. Dr Briscoe: I can quote from at least three case law examples that make it absolutely clear that the judge considered autism and the behavioural disability that arose from it, in those cases, to be covered by the DDA. I do not want to talk about social security benefits because they are not in our remit. However, it is our understanding that, when applying for benefits, what is important is the need of the individual.
1009. The Chairperson: Tim Moore's paper, which we will consider at 2.00 pm, will look at that important issue.
1010. Mr Gardiner: Thank you for your presentation, Dr Briscoe. We are all concerned about children with autism and we want the best for them.
1011. Dr Briscoe: As do we.
1012. Mr Gardiner: If an autistic child is admitted to hospital, will specialist care be available or will there be someone there who has been trained to look after the child?
1013. The Chairperson: Sam, that is an important point that should be discussed under the next clause, but it has absolutely nothing to do with clause 1.
1014. Mr Gardiner: OK, I will keep it for the next clause.
1015. The Chairperson: I suspect that I know the answer. I will let you in second when we move on, but I do not think that the definition of the DDA would have any impact on how a child would be treated in hospital; that would depend entirely on his or her condition.
1016. Dr Briscoe: I am sorry; I did not hear that.
1017. The Chairperson: Sam asked whether special treatment would be available for an autistic child who was brought to hospital. Treatment would be based on the condition of the child rather than on any definition —
1018. Dr Briscoe: If a case was complex and involved comorbidities one of which was autism, there would be a full care plan based on the needs of the child at the time of its admission to hospital.
1019. Mr Gardiner: There is no need to call me again, Chairman; I have the answer. Thank you.
1020. The Chairperson: Is your question about the DDA, Pól?
1021. Mr Callaghan: It is very specific to the DDA. Thank you for coming before us once again. We tested some of the issues last time; therefore I do not plan to rehearse them. They are in Hansard for everyone to enjoy or otherwise.
1022. Did both the case law examples that you mentioned relate to education?
1023. Dr Briscoe: They were both behavioural cases.
1024. Mr Callaghan: Did they both relate to access to educational services provided by the state.
1025. Dr Briscoe: Yes.
1026. Mr Callaghan: Is the Department aware of any case law — and since you represent the Health Department, let us stick in the silo mentality for a wee second — on access to health or social care services that demonstrate that the DDA definition covers ASD?
1027. Dr Briscoe: The DDA is not about health. [Interruption.] It is anti-discrimination legislation. The question is whether autism is covered by anti-discrimination law, regardless of the setting in which it finds itself. Our view is that it is.
1028. Mr Callaghan: Obviously, the — I am sorry, Chairperson, but there is some distraction.
1029. The Chairperson: We welcome members of the public, but interruptions can distract members and witnesses. I know that people feel passionately about the Bill, but please try to keep quiet so that the witnesses can give their evidence without interruption.
1030. Mr Callaghan: I am happy to come back to it in the afternoon. We can test it in other ways.
1031. Dr Briscoe: My colleague has just reminded me that there is case law in respect of DDA through employment tribunals and the impact on employment. There was a case recently that was much bigger, but its underpinnings related to autism. There was a case in the Health Service, but it was not directly about autism. However, the judge clearly said that autism was covered by the DDA.
1032. Mr Callaghan: If the Department is making that submission, it would be helpful to have case law references.
1033. Dr Briscoe: I can give you the Hewett case reference now. It is UKEAT/0526/03/ILB.
1034. Mr Callaghan: This is a composite point on the DDA clause: does the Department not think that it would be helpful to take the consideration and testing of ASD under the DDA definition at present and remove it from the sphere of judicial interpretation entirely to provide clarity?
1035. Dr Briscoe: The proposed definition is not related to autism but to "social (including communication)" and "forming social relationships", which is a much bigger. The connection between clause 2 and the amendment to the DDA is not real as the latter is a stand-alone amendment.
1036. There are at least three examples in the guidance on autism from the Office of the First Minister and deputy First Minister, including Asperger's syndrome and a child and an adult with autism, that clearly indicate that autism is covered by the DDA.
1037. Mr Callaghan: There are different views. The view that has been expressed by the Department is not held universally. You are entitled to your view as a Department, but it is not universally held. We are talking about judicial interpretation, but a judge would also interpret the context in which the DDA amendment came forward, which, in this case, is as part of an Autism Bill. We dealt with that before and we agreed to disagree. We will leave it at that.
1038. Dr Briscoe: You are obviously right to say that that is the view of the Department. As was stated previously, the responsibility for anti-discrimination legislation rests with OFMDFM. Although our view is informed by legal advice and so on, you would really need to seek the view of the Office of the First Minister and deputy first Minister if you still have concerns about the coverage of anti-discrimination law.
1039. The Chairperson: Assuming that no one has anything more to ask about clause 1, we will move on to the strategy and cross-departmental co-operation. Obviously, as MLAs, we have received a huge volume of correspondence and representations on the Bill. Other members and I have met numerous groups that represent the needs of autistic children, mostly, but also adults in the Province. There is a huge sense of frustration about the present service delivery. There are cries of help from parents who, frankly, cannot cope with the huge demands that are placed on them while looking after one or several autistic children. They support the Bill because they feel that it will force government to take autism seriously and drive forward real programmes that will meet their needs.
1040. You and the Department of Education seem to indicate that everything is fine because you are doing your best and you are delivering what you think is a suitable programme. However, the service users feel that there is an enormous chasm because of a lack of delivery. That is why there is such strong support for the Bill. How come there is that huge difference between the two viewpoints?
1041. Dr Briscoe: First, as my colleagues from the Department said, there is always room for improvement in any service. We recognised that and brought forward an autism strategy, an action plan and additional resources. Everyone would, of course, like additional resources. However, do we want to target resources at front-line services or do we want to divert them to bureaucracy and so on through the Bill?
1042. The question has resonance for me in that the implication is that the objective of the Bill is to give rights to individuals with autism to meet their needs, which includes children, parents and carers. If that is so, that objective is not clear in the Bill. In contrast, the Autism Bill in England is set out very differently. It outlines improvements to service provision and contains guidance on what that means. Our concern is about clauses 2 and 3 and that, as it is currently drafted, the Bill's objective may not be clear. If the Bill's objective is to, in some way, give individuals with autism rights beyond those of a person with another disability — Scotland talked about "two-tierism" — people with autism will be the beneficiaries of legislation whereas people with other disabilities may not be. How does that fit with article 14 of the European Convention on Human Rights?
1043. The Chairperson: We have heard glowing reports from the Department of Education about what it is doing. You emphasised what you are doing and have told us all about the wonderful co-operation between the various Departments. If that is happening, what is wrong with a Bill that simply brings that wonderful co-operation and all those strategies into legislation? As the Deputy Chairperson said, that will not do any harm.
1044. Dr Briscoe: My previous point was that it could potentially do harm. Depending on how we interpret clauses 2 and 3, those who live with autism will be beneficiaries of legislation that underpins a strategy and, in some way, will have a right to have their needs met. Therefore, that begs the question: what about the human rights of all other people with disabilities? What is the Committee's view on that? How could that position be justified against a challenge under the European Convention on Human Rights?
1045. The Chairperson: The Bill asks you only to draw up a cross-departmental strategy.
1046. Dr Briscoe: That is an interesting interpretation. If that is the Committee's interpretation, the other argument is that a strategy will not, in itself, necessarily improvement front-line services.
1047. The Chairperson: You question the competence of the Assembly to create a cross-departmental strategy. I cannot understand that. Your submission questions whether the Bill is competent at all.
1048. Dr Briscoe: I questioned clauses 2 and 3 only.
1049. The Chairperson: They are fundamental clauses. You questioned the competence of the Assembly.
1050. Dr Briscoe: I questioned its competence to legislate on this.
1051. The Chairperson: Health matters are entirely devolved. There are no reserved matters.
1052. Dr Briscoe: The Committee should consider the intention of clauses 2 and 3 and whether there are any issues or potential interference with the European Convention on Human Rights.
1053. The Chairperson: Yes, that might question the wisdom of having the Bill, but the competence test is normally whether we are within our legal rights to do it. These are bread-and-butter devolved issues; none of this impinges on Europe or on Westminster. You may say that Mr Bradley may not be very wise in sponsoring the Bill, but I cannot understand how you can say that it is not a competent Bill.
1054. Dr Briscoe: Perhaps a legal definition of competence needs to be brought, but it is our view, informed by legal advice, that there would need to be careful consideration of clauses 2 and 3. There is no issue about the competence of clause 1, but there are, potentially, issues of competence with clauses 2 and 3 because of what I said about clarity of intent, language and the potential interface with the European Convention on Human Rights. That must be considered carefully.
1055. The Chairperson: Our Business Office, draftsmen and legal folk have all looked at that, and they think that it is absolutely watertight. They have said that the 1990 Act enables us to produce legislation on the subject.
1056. Dr Briscoe: Bills are competent only if they are in compliance with European conventions.
1057. The Chairperson: We will go back and check that.
1058. Dr Briscoe: That is our view. Obviously, you will need to consider that.
1059. The Chairperson: The best brains in here would differ with you on that. Talking of best brains, John McCallister is next.
1060. Mr McCallister: That was a seamless introduction. Not to split up the Chairperson's compliment, I agree with a huge volume of what he said. Some of the earlier arguments against clauses 2 and 3 were that what the legislation proposes is being done anyway. I wonder why you object to clauses 2 and 3 and dispute their competence when you say that a lot of those issues are being pursued anyway in your strategy. Given that you are doing that in your strategy, how do you make the case that the Bill would add so much to the bureaucracy in the system? It means that you would have to co-operate with other Departments, but surely it is easier to get cross-departmental agreement than cross-party agreement. You have your strategy completed, and the Department of Education is also working on it. Is a lot of that not in place? You can tie in other Departments, including the Department for Employment and Learning and the Department of Justice, to do that. Where would the extra bureaucracy be?
1061. Dr Briscoe: For starters, we would have to develop a new strategy when we already have one.
1062. Mr McCallister: Presumably, you could lift a huge amount of your new strategy from the existing strategy.
1063. Dr Briscoe: We would have to put in a cross-departmental infrastructure to do that, and that in itself would cost money. There are fundamental issues about one Department monitoring another in the way that the Bill identifies. We secured an action plan and secured the resource for it, and we feel that we have an appropriate infrastructure that interfaces with education.
1064. As you saw in the paper, additional money, albeit a small amount, was set down for adults with autism. There are the beginnings of a uniform diagnostic pathway for adults. Clearly, more needs to be done for adults, and, in the care planning for adults, there are issues about how an individual might live independently in society. Those issues are part of the care planning process in relation to interface with employment agencies, housing and so on. We do not need legislation. As colleagues said earlier, it will not help us to improve service provision.
1065. Mr McCallister: The Chairperson's earlier point is right: if all of those things were happening, a huge lobby would not be saying that the rights need to be enshrined in law, which would force agencies to work together. If that were happening, a lot of the people who are sitting behind me would not be at Stormont today, and we would not be having this discussion.
1066. Dr Briscoe: I fully understand that autism is a big topic and is very important. The fact that we were one of the leaders in bringing forward an action plan means that the Department recognises that it is a very important topic. However, the Bill will not help us, particularly if the intention and objectives of clause 2 and clause 3 are not clear. It will not help us to do our job better. We have systems to communicate with other Departments as required. I fully acknowledge that there is more to be done, but legislation alone will not help us. A strategy alone will not help front line provision. In contrast, although there was a particular policy rationale for the English strategy, it is about improving service provision, and it clearly sets out how to do that. However, the Bill's objectives are not clear, and then there is the issue of —
1067. The Chairperson: Is that not, then, an argument for beefing up the Bill to include the English model of service provision and —
1068. Dr Briscoe: As I said, any Bill that goes forward has to have a clear policy rationale. In England, the policy rationale was that the Secretary of State for Health had no jurisdiction in respect of local authorities, gathering data and so forth. England does not have an integrated health and social care service, so there was a clear policy rationale in bringing forward an Autism Bill. It should be noted that that was for adults only; there is no Bill for children.
1069. We have an integrated health and social care system, so we do not need legislation to foster good relations across Departments or at local level. For evidence of that, John, look at the care pathway that was developed recently by the regional ASD group for children. It clearly refers to youth clubs, play groups and all of the other things that are important to children on that care pathway. Stephen Bergin is on the five-board education and library board group on autism. The regional ASD group includes linkages with education, employment and housing. It is not perfect, and nobody is saying that it is. It can always be improved. However, legislation will not help us to do that.
1070. Mr McCallister: I take it, therefore, that the Department does not propose any amendments to beef up the Bill or set it in the context of that policy background?
1071. Dr Briscoe: As I said in the paper, from our perspective, there is no policy rationale for the legislation.
1072. Dr Deeny: I have taken on board what you are saying. I have worked as a professional with people with all disabilities for 30 years now. Every one of them needs our full support in health, education and in legislation. I noted your concerns. Scotland talked about having two tiers in autism-specific legislation. Would this Bill be setting a precedent? Would it be the first disability-specific legislation, for example?
1073. I take on board and share your concerns. I work with a number of people with cerebral palsy and Down's syndrome. Are they likely to say that they should have a Bill to support them as well? I am just trying to tease that out. I was going to ask you about what was done in England, but you have partly answered it. There is a Bill in England, but I had forgotten that there is not one for children. I was going to ask you whether you would support a Bill such as that in England, but I think you have answered that. Why do you think they approved a Bill for adults but not for children in England?
1074. There are a few questions there. Would it set a precedent for other people who are equally disabled and who I know and work with to say that they will seek legislation for their disability and get their own specific Bill? Is that a concern for the Department? Secondly, why did Scotland not approve its legislation by a huge margin? Thirdly, why did England not proceed with an autism Bill for children?
1075. Dr Briscoe: I cannot answer the latter question on why the Bill in England does not cover children specifically. However, in my view there was a clear policy rationale for introducing an adult Autism Bill in England, particularly given the fact that they do not have an integrated health and social care system. That is in contrast to here, where, in my view and my Department's view, there is no policy rationale for doing that. As you have said, we are doing work; we do not need legislation to progress that work.
1076. You are right in saying that, in Scotland, it was felt that bringing in an autism strategy would not in itself improve front line services. That was one issue; the second was the issue of two-tier legislation. This Committee will need to give due consideration to that and to human rights. Article 14 of the European Convention on Human Rights deals with protection against discrimination. As I understand it, that includes a whole lot of things, such as protection against discrimination on the grounds of sex, religion, etc, "or other status". My understanding is that autism is included in that "or other status". In that sense, and given article 8, which deals with the impact on the individual's private and family life, it might be argued that individuals with autism might have greater protections because they are included in "or other status".
1077. I share your concerns about people who have other, perhaps more disabling, conditions. Are they not also entitled to that protection? Potentially, autism might be a beneficiary because it is underpinned by legislation, whereas other conditions might not be.
1078. Mr Callaghan: The business of the hierarchy is obviously important, but I think people may be getting a bit carried away. You put it to the Chairperson — I hope I am not misinterpreting what you said — that you took it from some of the things that have been said that the objective of the Bill is to meet the needs of people with autism. In a way, I am not sure that that is what clauses 2 and 3 of the Bill actually purport to do. Clause 2 effectively purports to improve co-ordination by imposing statutory duties, and clause 3 purports to set out how needs will be addressed. That is not quite the same thing as giving a statutory guarantee that needs will be addressed in every circumstance.
1079. What would you say to people who will argue about whether the particular needs of people with autism are being met? Those needs were clearly demonstrated to us by the autism community and lobby. If you give Cinderella a ticket to the ball, it does not mean that everybody else has to leave the ballroom. It just means that Cinderella gets to go to the ball.
1080. Mr Easton: He is not asking you to dance by the way.
1081. Dr Briscoe: He gave the analogy of a nightclub the last time we met, so I am just thinking through what he has said about Cinderella. Obviously dancing is a big issue.
1082. Mr Callaghan: Dr Briscoe, I have become a father since the last time we met, so maybe I am becoming a bit more Disney-like in my aspirations.
1083. Dr Briscoe: Wales is often held up as the exemplar in respect of developing a strategy, but it did not need any legislation to do that. In fact, it still does not have any autism legislation. Therefore, we question the need for legislation. We do not need it in order to move forward. Some individuals in the discussions will quote from the Welsh example of how to develop a strategy, but Wales does not have any legislation underpinning that.
1084. Clause 3(1) states:
"The autism strategy must set out how the needs of a person with autism are to be addressed throughout their lives."
1085. Therefore, it is a matter of the interpretation and the absolute understanding of the objectives of clause 3 in its entirety. If you go for the former, that the objective is that the rights and needs of individuals are to be met, potentially the rights of other individuals could be called into question. If you take it that it is a strategy that just does what it can, it does not say that the strategy has to improve service provision. If you argue that that is what the strategy is intended to do, the Bill states that it is without significant additional cost. For me, there are issues on reconciliation of the argument in relation to clauses 2 and 3, depending on what you consider the objective to be.
1086. As we indicated to you, we do not believe that the Bill has no significant cost. Indeed, we believe that it will divert resources from front line services. I am trying to answer the question on Cinderella without actually referring to her.
1087. The Chairperson: To follow on from that, the accusation was made that if you develop a strategy for autism, others will come to the table demanding similar treatment. The autism lobby will say that there is absolutely no evidence of that actually happening, because autism is such a special set of circumstances involving such complex needs and encompassing so many Departments. Lobby groups representing other conditions such as ADHD or Down's syndrome are not demanding a similar type of treatment. Therefore, they all go to the ball, rather than anybody being excluded.
1088. Dr Briscoe: I have to challenge that. I do not want to go into specific conditions, but there is a broad range of specific conditions, such as multiple sclerosis, muscular dystrophy, and a lot of neurological conditions, and the whole Bamford ethos indicates that there is a range of conditions that want considerable improvement in service provision. The fundamental basis of the Bamford review, which covered mental health and learning disability, was that there was recognition that there was a long way to go in respect of enhancing provision and that it was underfunded in relation to the rest of the UK.
1089. The Chairperson: You frequently mentioned Scotland and Wales. Due to the nature of the Northern Ireland Act 1998, we have ministerial Departments and a mandatory five-party coalition. Therefore, we have 12 or 13 silos, and, for obvious reasons, people will jealously guard the boundaries of those silos. In Scotland, there is a novel concept of not so much ministerial posts but themed Departments, which cover the specific needs of children or the elderly, etc. It is a very forward-looking way of doing things, but it would not work in this country for at least the next century because of the tribal nature of the way in which we live.
1090. Equally, in Wales, there is no mandatory coalition. There is a one-party Government with minority support, which means that it is much easier for Departments to work across boundaries. Do we not need something in Northern Ireland that will legally force our Departments to co-operate, given the nature of the settlement that we have here? With all its flaws, I think that it is the only one that we will have for a long time.
1091. Dr Briscoe: We believe that we have all the legislation that we need to work across Departments, and we can provide you with evidence to that effect. All you have to do is look at some examples, such as the inter-ministerial group on Bamford and the inter-ministerial group on domestic and sexual violence. There is a range of public health issues concerning children, and Dorothy Angus mentioned the OFMDFM subcommittee on children and young people. Therefore, there is a range of examples of how Departments work together. I will say again that we do not need legislation.
1092. The Chairperson: On what basis do you make the assertion that the objective of clauses 2 and 3 are not clear?
1093. Dr Briscoe: I have tried to explain that.
1094. The Chairperson: I am not 100% certain that I understand.
1095. Dr Briscoe: OK. You started off by asking something along the lines of, is the objective that the needs of persons with autism should be addressed? If that is the objective, it makes autism and people with autism beneficiaries of legislation, whereas other people who have equally disabling conditions will not have that. If that is the objective, we believe that there are issues there, especially as autism is a spectrum disorder. There are issues in respect of other client groups and other people with significant disabilities.
1096. If the objective is to write a strategy that endeavours to do something to raise awareness of autism, a strategy alone will not improve front line services. That is particularly the case when the Bill states that there are no significant costs attached.
1097. The Chairperson: Clause 3(1) states:
"The autism strategy must set out how the needs of a person with autism are to be addressed throughout their lives."
1098. Is that not clear?
1099. Dr Briscoe: I am saying to you that, if that is the objective, what about other people who have equally disabling conditions? What about their ability to have additional benefits in legislation that people with autism will have by virtue of the Autism Bill? Therefore, it depends on how you interpret clauses 2 and 3. One would need to be sure that clauses 2 and 3 are compliant with the European Convention on Human Rights, with particular reference to articles 8 and 14, as I have already indicated.
1100. Mr Easton: I am sorry that I missed part of your presentation. I like you, but I do not like you enough to go to the ball with you on this issue.
1101. The Chairperson: I do not know how you will interpret that statement. A mobile phone is switched on, and it will interrupt the recording.
1102. Mr Easton: What I like about the Autism Bill is that its strategy involves all Departments. Does your strategy involve every Department?
1103. Dr Briscoe: It is designed primarily for health and social care. There are five themes in the strategy, and the last theme relates to engagement and partnership working. A number of actions under that theme promote inter-agency working. We specifically put that in there because we recognise the importance of inter-agency working. Therefore, we are trying to build on what we have, improve our services and, as we develop, the interface with other agencies — I gave the example of the care pathway for children — and the commencement of additional services in relation to adult diagnostic services.
1104. I want to bring in some of my colleagues on this issue. In respect of care planning for children, inter-agency working is fundamental, regardless of whether it relates to autism or not.
1105. Mr Charles Bamford (Department of Health, Social Services and Public Safety): Yes, indeed. There have been a number of recent improvements, which we have already mentioned. I am not too sure what the advantages would be of compelling something to happen through legislation. There is already a degree of accountability for staff on the front line, and that accountability is leading to improvement across agencies, not just in the statutory sector but in voluntary organisations.
1106. Social care staff and social workers in particular are very sensitive to the needs of parents and look at providing support mechanisms for parents by way of timely information and good communication across the education and housing sectors, so that an adequate care pathway is provided for their sons or daughters. I fully recognise that there are huge pressures out there. I also recognise that staff are saying that there have been significant improvements. There is still a lot to be done, but there is now accountability and recognition that the issue needs to be profiled in the future.
1107. Mr Easton: I accept that your strategy will work with some agencies, but can you guarantee that every Department is working with you on autism issues?
1108. Dr Briscoe: We have produced our strategy, but our job relates to policy. The implementation of our policy, which is on the action plan, is the responsibility of the regional ASD network group in collaboration with the local fora, which I am sure you will have heard about from Stephen Bergin. Therefore, our job is not implementation. Our job is policy. As has been stated, we recognise the importance of inter-agency working, and we will continue to do that. We have strong interfaces in lots of areas, and we meet regularly with our colleagues from the Department for Employment and Learning (DEL) and the Department for Social Development (DSD). We have a good interface there at policy level, but the outworkings of our action plan are through the ASD network group. I suggest again that you look at the children's diagnostic care pathway if you have not already done so. Stephen and others worked on it, and it will show you that there is wide inter-agency work.
1109. Mr Easton: I accept that you are involving other agencies, and you are trying to pass the buck to somebody else who will deliver the strategy, but I am looking for a cast iron yes or no. Does it involve every Department?
1110. Dr Briscoe: We interface with every Department.
1111. Mr Easton: On autism?
1112. Dr Briscoe: Yes, as we need to.
1113. Mr Easton: As you need to?
1114. The Chairperson: There might not be a huge interface with Departments such as the Department of Agriculture and Rural Development (DARD).
1115. Dr Briscoe: These things are not just about autism; they are about disability in the round. It is very important to hold onto that. For example, we are developing a physical and sensory disability strategy, which is nearing completion. In that context, we have interfaced with DARD, recognising the importance of transport, housing and employment issues, and so on. Therefore, it is about how we look at disability in the round. We recognise and interface with all Departments as we need to.
1116. Mr Easton: It is commendable if you are doing all of that, but does that mean that the other Departments will train all their staff who deal with the public on issues that they will have to face when they deal with people with autism? Can you guarantee that all Departments will do that?
1117. Dr Briscoe: I am glad that you brought up the training of civil servants because there is a lack of clarity around that issue. The Bill states that all civil servants who deal directly with the public will be trained. It is interesting that, in a previous iteration, it was about training public sector staff. It could potentially cost £1·8 million to give civil servants autism awareness training. However, is that the right training? What does "Civil Service staff" mean in this context? Would it not be better to train front line staff, such as doctors, nurses, etc, and to widen that out into other areas? There must have been good reason for the sponsor to change the wording from "public sector" to "Civil Service". I do not know the reason for that, but, either way, there is a substantial cost to that. Training civil servants will not impact significantly on front line service provision.
1118. Mr Easton: Finally, I would have thought that it would be beneficial for staff who deal with welfare and benefits to get that autism awareness training. I think that that type of training is important. It is equally important that people with autism who apply for grants to set up their own businesses get help to do that.
1119. Dr Briscoe: We talked about the DDA earlier, and we said that this is our Department's perspective. You might wish to take advice from the Department for Social Development in respect of benefits and access to benefits, etc.
1120. The Chairperson: I will let Pól ask one more question because no one else has indicated that they wish to speak on this section. We are running slightly over time, so this will be the final question.
1121. Mr Callaghan: I am sure that the Chairperson will be happy if the precursor to my question is a request for more information on how much training the £1·8 million that you mentioned would deliver, who it would be delivered to, and your definition of who deals with the public. That is interesting for considering the clause and sub-clause.
1122. My question is on costs in general. As you portray it, the monitoring requirements of the Bill would create unnecessary bureaucracy. Has the Department assessed what the costs would be? You told us that there is a lot of collaborative work going on, and you talked about the mechanisms behind the care pathways, care planning, interdepartmental work, inter-ministerial work, and subcommittees and everything else. If the collaboration were more streamlined, presumably there would be cost advantages to that.
1123. Drilling down into the actual substance, one of the points behind the Bill is that better co-operation does not, ipso facto, lead to more cost. It can actually lead to savings. One of the complaints that we are getting is that there is almost too much overlap and duplication. Different agencies are trying to do different things with the same objectives, rather than having high-level aims, and there is frustration on the part of some families that one hand does not know what the other hand is doing. Therefore, presumably, there would be better savings if there were better co-ordination.
1124. I appreciate that some of that seems to be because, for good reasons, different Departments have tried to ramp up over a reasonably short time and in a historical context over the past few years. Therefore, it is a case of everyone getting out into the field. You are firing shots and so is the guy beside you, but, maybe if you have the one target, you would fire fewer bullets. That is a horribly anti-pacifistic analogy. There is a question in there somewhere.
1125. Dr Briscoe: In relation to your first question on civil servants, we estimate that, based on 25,000 civil servants, it will cost £65 each for training, which would lead to a training bill of £1·8 million. In one way or another, civil servants deal — and the word "deal" is in the Bill — with lots of people, but is it appropriate that we spend £1·8 million in training civil servants who deal with the public? Even if £1·8 million were available, at a time of budgetary constraint, would it not be better to train public sector workers in front line service provision — people who work in local councils, in the Housing Executive, doctors, nurses, social workers, the PSNI, and the broader range of public sector workers — rather than civil servants.
1126. This is a time of budgetary constraint, and, from meetings with colleagues in the Department, you will be aware of our financial position in respect of the global finances of the draft settlement. The Bill is not without cost. Where will that money come from, and is it an appropriate use of money to train civil servants at a cost of £1·8 million? We have given you a minimal and a significant cost in respect of what the public awareness campaign might be. Again, that is a significant cost.
1127. As regards your second point about interface with Departments, you asked why we do not streamline our interface, but the Bill is asking us to create an infrastructure specifically for autism. We interface on a number of issues, such as public health, and there are a lot of issues in there on Bamford, on mental health and learning disability, and the whole range of conditions in that. Equally, we have a lot of discussions on physical and sensory disability, yet you want us to create another bureaucratic layer specifically for one condition.
1128. In saying that, I want to emphasise to colleagues in the audience and to the Committee that the Department is absolutely committed to trying to improve autism services. That is our aim, but we honestly do not believe that the Bill will assist us to do that. We have all the legislative power that we need, and we do not need any more.
1129. The Chairperson: Thank you very much. I am sure that your colleagues are annoyed that they did not get an opportunity to speak.
1130. Dr Briscoe: I was just going to ask whether Ian and Peter would like to say something.
1131. The Chairperson: I was only being facetious. They actually look quite relieved that they were not asked to speak.
1132. Dr Briscoe: The Bill has clinical implications. We talked about clause 4 the last time, and there were important issues in respect of definition, etc, and we still hold that view. Ian was very articulate on that the last time.
1133. The Chairperson: Unfortunately, we have run out of time, but thank you very much, Dr Briscoe and your team, for your helpful information.
20 January 2011
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Mickey Brady
Mr Pól Callaghan
Dr Kieran Deeny
Mr Alex Easton
Mr Tommy Gallagher
Mr Sam Gardiner
Mr Paul Girvan
Mr John McCallister
Ms Sue Ramsey
Witnesses:
|
Ms Laura Collins |
Regional Autistic Spectrum Disorder Network Reference Group |
1134. The Chairperson (Mr Wells): The witnesses are led by Lord Maginnis of Drumglass and are from the Regional Autistic Spectrum Disorder Network (RASDN) reference group. Once again, I remind members of the public and Committee members to turn off all mobile phones. It is particularly difficult for witnesses when mobile phones ring. Please allow the witnesses to make their presentation without interruption. Lord Maginnis, who is known to most of us, is the chairperson of the RASDN reference group. Laura Collins is a parent care representative, and Nuala White is a parent.
1135. Lord Maginnis (Regional Autistic Spectrum Disorder Network Reference Group): Do you mind if I take my jacket off?
1136. The Chairperson: No problem, Ken. You are back to your old stomping ground of 1982 to 1986, so you should know the routine here very well. Normally, we ask witnesses to make a brief opening presentation of around 10 minutes, and there will be questions for around an hour. You are very welcome, Ken, and I am sure that you will have no problem handling this session.
1137. Lord Maginnis: Thank you, Mr Chairman and members of the Committee, for having us here. After a long wait, a sudden summons came that we should arrive with you, and we are pleased to be here. With your permission, I intend to outline briefly my involvement, and then Laura and Nuala will tell you about themselves. Similarly, so that we know the extent to which we have to go into detail, I would like members to indicate whether they have read the independent review of autism services. I know that they have had a multitude of papers.
1138. The Chairperson: The majority of members have probably not had the time to read it all. All that we have had is summaries and press reports on it.
1139. Lord Maginnis: Indeed. We will keep that in mind. As you know, I have been involved in public life for around 30 years. Around 16 years ago, under direct rule, I began to take an interest and to talk to Ministers in the Northern Ireland Office about autism problems. It was not something that I knew a great deal about, but I did that simply in response to parents explaining the situation to me. I learned that there was no formal structure and no one with overall responsibility for autism in the Northern Ireland Office. Later on, about nine years ago, I discovered that a member of my family was on the spectrum, so I have had nine years of living cheek by jowl with that.
1140. When the current Assembly was formed and sitting, I spoke to the Minister of Health, Social Services and Public Safety and suggested that he should take an interest. I am grateful to say that he responded very positively. I finished up, for my interference or for whatever other reason, chairing the independent review of autism services, during which we took a great deal of evidence, sitting around the table with half a dozen experts. The Department of Health, Social Services and Public Safety (DHSSPS) subsequently asked me to chair the regional reference group. It is difficult but necessary to have a comprehensive group, given that we have five health trusts. It is important that we have groups that can interface with each of the health trusts and co-ordinate a programme so that people who live in Castlederg have the same opportunities as those who live in Newtownards or Coleraine. That has taken time.
1141. There is a group of 30 people, consisting of parents, carers and users, who work together and who have addressed the issues as they know and experience them. They interface with the health trusts. I will now let my two colleagues tell you who they are and what their experience is.
1142. The Chairperson: We are particularly interested in the Bill. We have had copious evidence on the concerns of those who care for autistic children and adults. That is a major issue in itself, but we are particularly interested in the relevance of those concerns to the Bill.
1143. Lord Maginnis: I fully understand that. The group wants to give the Committee an idea of where it is coming from and of our hands-on experience. We will certainly address the issues in the Bill.
1144. Ms Laura Collins (Regional Autistic Spectrum Disorder Network Reference Group): I am a registered adult nurse and a registered sick children's nurse. I have a BA from Queen's University Belfast in business and management. I have been a family carer for 30 years. I have cared for five members of my family: learning disability, autism — my son is approaching 30 — mental ill health, dementia, brain injury and cancer. I have been a carer–activist over that period, championing the support needs of disabled people and their carers.
1145. I have 40 years' experience in the voluntary and community sector and have been involved in more than 30 organisations. I have been involved with nearly every one of the autism charities in Northern Ireland and was a founding member of the original one. I have represented carers' views in an official capacity: I sat as a carer representative on the disability living allowance (DLA) advisory board from 2001 to 2005; I was a regional counsellor with the National Autistic Society between 1993 and 1997; I was a carer representative on Crossroads Care management committee between 1990 and 1996; and I was a Carers UK trustee with 18 years' active engagement with Carers Northern Ireland. I am a member of several strategy groups in my local trust. I am the facilitator for the Belfast area of the reference group.
1146. Ms Nuala White (Regional Autistic Spectrum Disorder Network Reference Group): Hi, guys; I am glad to be here. I am nervous, so you will have to bear that in mind. We will give the Committee summary documents when we have covered all the areas that we intend to speak about so that you do not have to take copious notes. We will talk about the handout that we gave you in advance in just a second.
1147. I have been an ASD parent carer for the past 16 years: my son turns 16 tomorrow. As a parent carer, I am in family crisis at present, but I am still here working from a different angle. I live with autism, so I speak with some authority, although I do not intend to major in it.
1148. I have a masters in autistic spectrum disorders from Queen's University Belfast. The particular experience that I bring to the Committee's meeting, to the reference group and to the whole debate on legislation is that I am a fellow of the Chartered Institute of Personnel and Development. I specialise in organisational and whole-systems change around what it takes to make successful transformation happen. I have significant experience in the Scottish Government and with Irish health. I am a practising psychotherapist counsellor, and I provide support to autism families. I am a reference group member with the South Eastern Health and Social Care Trust, one of the 30 to which Ken referred. We are happy to answer questions later about any of our roles and our experience. That puts us in context.
1149. I am aware that you have probably been swamped with submissions and written documents: we do not intend to add much to that. I would like to cover a few issues before we talk in detail.
1150. We are members of the reference group for RASDN. Among the 30 parents and 10 voluntary organisations, there are diverse views, ideas and experiences. We have never had a vote or debate specifically about who is for or against a Bill. We do the "roll up your sleeves" work in the field with all professional bodies and interested parties. We hold and can tolerate all those different points of view. We do not come here with a "for" or "against" stance; our purpose is to engage with you in dialogue about what will improve services for ASD parents, carers and service users; to explore with you in shared questions and answers the negative and positive effects that legislation might have on living out that strategy; and to inform the real living of the strategy in service provision. Are you with me?
1151. The Chairperson: I re-emphasise: we are talking about the Bill.
1152. Ms White: Absolutely, but we do not come with a "for" or "against" view. We want to put the issues in the context of some of the real work that is going on. We invite you to test us on the Bill around that, if you so wish.
1153. I will hand over to Laura to outline some of the input of our work.
1154. Ms Collins: The two main clauses of the Bill concern amendments to the Disability Discrimination Act (DDA) 1995 and the proposed strategy. I will address the strategy.
1155. In the RASDN reference group, we have been working extremely hard in response to the framework set up by government. I will quickly outline the achievements so that you can understand what the strategy looks like in action and what has been delivered. As parents, carers and users, we are at the very heart of the work. It is exceptionally new work.
1156. The Chairperson: The Committee has already heard that evidence from Stephen Bergin. Our problem is that a series of groups has come forward. Each has taken the opportunity to emphasise what it is doing on the needs of autistic children: that is fine. Our difficulty is that we are not reviewing autism services in Northern Ireland; we are looking at specific legislation. A recent set of witnesses never got to the point. It is vital that you move rapidly to your view on the Bill rather than giving an overall view of what is being delivered for autistic children. That is relevant but not to what we are currently undertaking.
1157. Lord Maginnis: Let me see whether I can help the Chairman and the Committee. As Laura and Nuala said, because we are involved, I suppose that we want to talk about what we are doing and how that has a practical impact and is an empowering exercise. We believe — I believe — that the Bill would disempower parents, carers and, obviously, users.
1158. I will turn to clause 1 and consider the two amendments to the DDA. The first states that, along with physical and mental impairment, we should insert the words "social (including communication)". I have already heard Tim Moore from the Assembly's Research and Library Services express his concern on that issue. It could — I believe that it will — be a constraining addition. It would constrain the definition that is already covered by "physical and mental impairment".
1159. There is another small amendment to paragraph 4(1) of schedule 1 to the DDA, which has a list running from (a) to (h). I then find that this Bill will insert:
"(i) taking part in normal social interaction; or
(j) forming social relationships."
1160. Those are not in the same grammatical form as the first eight points, which list:
"activities only if it affects one of the following —
(a) mobility;
(b) manual dexterity;
(c) physical co-ordination;
(d) continence;"
1161. and so on. Those are nouns. Tagged on the bottom will be something that is not a noun:
"taking part in normal social interaction;".
1162. I suppose that that could be changed simply to "social interaction", and "forming social relationships" could be changed to "social relationships".
1163. The point is simply that if we were all the same, nobody would be different. You will do things that I will not do, and I will do things that you will not do. If I am different from my peers or the rest of my family, am I somehow to be queried for having the wrong social reaction? Many people here may be teetotal, but if I do not go to pubs to drink, and my colleagues do, is there something wrong with me? If I am shy, is there something wrong with me? When defining autism, we must use much less generic terms than the Bill suggests.
1164. One of my biggest criticisms is that I read the Bill twice before I caught on that I was reading "the Department will" over and over, and it was only when I read the supplementary element that I discovered that "the Department" is the Department of Health, Social Services and Public Safety. Ladies and gentlemen, you know that the Department of Education will not be dictated to by the DHSSPS.
1165. The Chairperson: Ken, have you finished your objections to the Bill's amendments to the DDA?
1166. Lord Maginnis: Yes, I have. That will be taken up by Nuala.
1167. The Chairperson: We propose to split the questions. You have gone on past your 15 minutes already, and I must give members an opportunity to question you.
1168. Lord Maginnis: That is fine.
1169. The Chairperson: If that completes your evidence on clause 1, I will ask members whether they have questions on clause 1, and we will then move on to the strategy, which you were about to talk about, and we will ask questions on that.
1170. Ms White: Will we have an opportunity to give you some information to ground our debate?
1171. The Chairperson: Some of the information that you gave is not relevant to what we are doing. We are examining a Bill. All the witnesses have had the same problem; they have used the opportunity as a platform on which to bring up other issues about the care of autistic folk. That is relevant, but we specifically want to examine the Bill. That is why I am splitting the evidence in this way.
1172. Ms White: I am really sorry to come back on that. I would really like to have the opportunity to put to this body the question that we, as an organisation, are struggling with. It is an open question: how will the Bill help or not help, given what is going on at present and some of the cost realities. Will we have a chance to do that?
1173. The Chairperson: Yes, you will. However, this is about the Bill; it is not a review of general autism services.
1174. Ms White: Absolutely; we know that.
1175. Lord Maginnis: At the end of the day, Chairman, we want a result. We want a result that benefits the community and that meets the needs of those on the autistic spectrum. We cannot find — at least, I have not found — a methodology that allows us to examine that in limbo. We have to put it in context. We will leave it to you.
1176. The Chairperson: Alex is the first person who wants to question you on clause 1.
1177. Mr Easton: I am not sure that I want to now.
1178. I am a bit baffled, but I will set that aside. If the strategy is working so well, why do so many groups that are involved with the wide spectrum of autism want the Bill? Why do they feel that they need the Bill and that the strategy is not giving them what they want?
1179. The Chairperson: Alex, is your question about the DDA or the strategy?
1180. Mr Easton: It is a bit of both really.
1181. The Chairperson: As regards the DDA specifically, why do you think that so many groups said that they want the amendments?
1182. Ms White: That is a live question for us in the RASDN reference group. I can answer it only by telling you about the real work that is being done on the ground. No one has had the opportunity to tell you guys about that intense and thorough work. I can tell you about it in two minutes.
1183. The Chairperson: Is it relevant to the Disability Discrimination Act 1995?
1184. Ms White: It is relevant to the Bill. You asked a good question: why would a Bill be introduced? That is our working question too: what will a Bill add? We do not have the answer to that, given that we are living through very real change. We are living off an action strategy, which I believe clauses 2 and 3 deal with. The ongoing question is: how will a Bill add to, or interfere with, that strategy? May I give information on that?
1185. The Chairperson: Is it relevant to clause 1?
1186. Ms White: I do not know. I do not speak in clauses.
1187. Lord Maginnis: I will bring in Laura in a minute.
1188. Mrs O'Neill: Perhaps you are coming at this from the wrong angle. We are not here to attack the work of the group. Dr Stephen Bergin has been before the Committee. We are very much aware of the work of the network and the parents, users and voluntary groups involved. We have to look at it in clauses — that is our job as a scrutiny Committee. There are members of the network who support the legislation and feel that the DDA should be amended. Perhaps you can approach it from that angle. We do not dispute the good work that is done. Why do you think that members of the network feel that we should support the amendments to the DDA despite the good work that is done?
1189. Lord Maginnis: I heard Mr Easton's leading question. He mentioned the fact that groups support the Bill, but there has been no public consultation. Groups tend to do what they are told. There are some very domineering people in some groups. I have heard groups say that they represent 20,000 or 200,000 people with autism, which is absolute bunkum. Those groups are misrepresenting themselves, because they do not interface with anything like that number of people. Some of the groups work locally. Some are more concerned with whether their group will receive money from the DHSSPS to supply services than —
1190. Mr Easton: On a point of order, Mr Chairperson. This is not about attacking community groups or any other groups.
1191. Lord Maginnis: Indeed it is not.
1192. Mr Easton: I think that we need to stick to the DDA.
1193. Lord Maginnis: You were the one who said that you had a difficulty in understanding. I was trying to explain it to you.
1194. Mr Easton: You were being a wee bit all over the place, if you do not mind me saying so. Perhaps you could stick to the DDA question.
1195. Lord Maginnis: Would you like to ask your question again?
1196. The Chairperson: The question was: why are so many groups that represent the needs of autistic families and children so keen for the DDA to be amended to include a social —
1197. Lord Maginnis: Individuals want service, and I believe that that will slow it down. The wording of your Bill suggests that, if you agree to this, it will be two years before we implement a strategy. We are ahead of you by a year in implementing a strategy.
1198. The Chairperson: The "you", Mr Maginnis, is Dominic Bradley. We are scrutinising a private Member's Bill, and we have not come to a decision on it. It is important that you realise that this is not the Committee's legislation.
1199. Lord Maginnis: Sorry.
1200. The Chairperson: However, that was a relevant answer. Ms White, do you to come in to support that answer?
1201. Ms White: I want to answer the question. I do not deal with technical issues —I know that others do — but the clause in question expands the legislation to include "social (including communication)" alongside physical and mental disabilities. Families find it impossible to achieve service provision and to get the diagnoses and the interventions that they need. Naturally, they want the might of the law to support them in any way that it can to ensure that their young people or adults have the diagnoses that they require and can force the hand of service providers to meet those needs.
1202. You have discussed whether or not the expansion to mental and physical needs to be made. We do not have a collective view on that. However, I can support the notion that pinning the definition down further will make it more difficult, as somebody said earlier, for the likes of high-functioning people with autism or people with Asperger's syndrome to have their diagnosis held up. As Tim said earlier, expanding it makes it narrower, not broader. Therefore, people want the complete Bill to have some weight and to include a horse of Troy with which they can get diagnostic and intervention services to meet their needs.
1203. The Chairperson: I will not make any comment on your answer; it has hit the target 100%. That is the sort of answer that we require. You dealt with the issue very succinctly.
1204. Ms White: As a representative and given my experience, our response is that, when we consider a Bill, we determine whether the ongoing work is doing enough. With more support and joined-up government — I am sorry; I cannot separate it into different clauses — and if the Department of Health, Social Services and Public Safety, the Department of Education, the Department for Employment and Learning and other parties were to work together in support of the provision of autism diagnosis and intervention and the active joined-up work that is being lived out, there would, possibly, be no need for a Bill. I use the word "possibly", and I do not say that on behalf of 30 people in the reference group. I speak from my experience and knowledge.
1205. Dr Deeny: Do a significant number of carers and parents who look after people with ASD across the spectrum feel that clause 1 will make the situation worse and should not go ahead? Perhaps you do not know; I am not asking for figures. Secondly, as I said to Tim, I am concerned that, if we extend the clause and include the words "social (including communication)" it may apply to many groups of people. For example, I work with blind and deaf people. They do not consider themselves to be mentally ill but sensory-impaired. They may well say that those conditions should be added, but are we opening up a can of worms for the definition to apply to a whole list of conditions? Is your reference group happy that "physical or mental" — I dispute that it covers everything — is all-encompassing? Are you happy that it fulfils the needs of the carers of those with autism?
1206. Lord Maginnis: Not only are we reasonably happy with that but we have conducted research and know that the Equality Commission believes that, so far, cases that involve people with autism have been satisfactorily dealt with under the Disability Discrimination Act 1995. It appears to be the commission's view that autism is already embraced by the existing words. Tim Moore cited the Hewett case. Does that case stand alone and, as Tim suggested, not create a precedent? Is the Act adequate to his case? On that basis, the Equality Commission believes that clause 1 is flawed.
1207. Ms Collins: As far as I am aware, the Autism Act 2009 in England did not require the Disability Discrimination Act 1995 to be amended. Scotland's Bill has fallen, and Wales is delivering extremely well on its action plan. Wales has £7·1 million and, therefore, effectively twice our per capita investment.
1208. Therefore, strategic plans are enacted and working. There is sufficient legislation. The DDA is strong because it is broad. My concern is that we should not narrow it down, or the people whom we are trying to protect will lose out. Even the definition given in it is not the clinical definition in the International Classification of Diseases (ICD) 10 that is normally used for autism, and other syndromes are included. As was said earlier, we could end up legislating for absolutely everyone. The DDA already covers people who have autism, and there is no need to amend it.
1209. The Committee has received many presentations. Not every autism-specific charity supports the Bill, and the Committee may not have heard evidence from them all. The disability sector's position is neutral. It will not be championing something that could split it, in that one disability may have pre-eminence over another.
1210. My other comments are to do with the disability aspect, which is extremely important. If we reach a point at which everything is about a medical diagnosis, that could be a retrograde step. We have moved so far into a social model, whereby we see the person first. It is retrograde to revert to labelling people, so that people without labels will not get what they want.
1211. The Bill does not address the issue of dual diagnosis — co-morbidity or co-occurring conditions. It is rare for someone to have pure autism. Some 50% of people with autism will have a learning disability, and similar numbers will have mental health problems, attention deficit hyperactivity disorder (ADHD), epilepsy and some 30 co-occurring conditions. Those people will not be supported. That is the complexity of autism with which we struggle. We are not dealing with just one condition but with many, which is why the regional strategy is pulling all the groups together. We have 10 voluntary agencies, which are not just autism voluntaries. There is Mencap, which provides learning expertise for the early years of learning disability. There is Barnardo's, which has early years guidance. We need people from many different areas and many different areas of expertise. That is what we struggle with. I do not feel that by being prescriptive that we are helping. It is important for those different groupings to work together, and we are doing that. They all bring their expertise to the table to design the services that families with complex needs require.
1212. The Chairperson: We are back to the territory that I was keen to get into.
1213. I will open up the session to include the second aspect of the Bill, which is the strategy and co-operation between Departments.
1214. Mrs O'Neill: May I make a point on the DDA?
1215. You said that the English legislation did not amend the DDA, but in England, the definition of disability under the DDA is being examined, and much work is being done, so it is recognised that we all need to consider that.
1216. The Chairperson: I can now open the meeting to other aspects of the Bill.
1217. Mr Callaghan: I would like to stay on the DDA for a moment.
1218. Lord Maginnis mentioned that the Equality Commission is not promoting the change to the DDA. However, it appears to me that the Equality Commission's proposal is for a more fundamental review of the DDA as it applies here generally: founded on a social model rather than on a medical one. That is a question for another day, I suppose.
1219. Tim spoke from the research side. It is important that we all recognise that Tim was putting forward various views for the consideration of the Committee rather than expressing a view, either on his own behalf or on behalf of the Assembly's Research and Library Services. He did not take a position.
1220. The Chairperson: He took no position. He is neutral.
1221. Mr Callaghan: The Research and Library paper states that the Equality Act 2010 in England, Scotland and Wales has guidance and that it refers to activities such as normal social interaction and forming social relationships. Therefore, those concepts that are to do with protecting capacity are in place in England as far as the guidance is concerned, rather than at primary legislative level. I am not sure how that rhymes with some of the concerns that you are expressing about the definition being too broad. You talked about what is normal and what is not normal and the rest of it. What is your view on that?
1222. Lord Maginnis: I am not here to try to explain the medical definition. I am not a medical person, nor have I ever pretended to be. I run things, I chair things —
1223. Mr Callaghan: I am not asking you to do that, but to be fair, Lord Maginnis, perhaps I mistook you. My interpretation of what you said to the Committee is that you drew particular attention to clause 1(3) of the Bill, which inserts at the end of paragraph 4(1) of schedule 1 to the Disability Discrimination Act 1995 the following:
"(i) taking part in normal social interaction; or
(j) forming social relationships."
1224. I distinctly remember your talking about the grammatical construction of the amendment. My understanding of what you were saying is that that was almost going into the realm of the absurd and that it was a case of legislation taking a view of what is normal and what is not normal. I am making the point that in England, since last year, guidance has been in place relating to the Equality Act 2010 that specifically covers those activities. It is also probably useful for us to remember that the threshold for activities to be covered has to be met. It is not the case that any old problem with, for example, social interaction, would be covered. There is a threshold that has to be reached before the test is met. Do you think that the guidance in England has created a problem since it was put in place?
1225. Lord Maginnis: We all know that there is a difference between guidance and legislation. There is a difference between that which is aspirational and that which is substantive content. There is no answer to your question. We are discovering day in, day out that there are special needs. It is about enabling people not only to be aspirational — to want to treat the needs of all the people on the spectrum — but to get down to the substance of the issue. It is about having links and pathways. We use the word "pathway" quite a lot. You will understand that. We are trying to create pathways that cannot possibly be legislated for. However, if we base what we are doing on the Disability Discrimination Act 1995, we will be continually creating guidance, whether it is for GPs, therapists or whomever, and doing that at the coalface.
1226. I will repeat my criticism of the Bill. It requires the Department of Health, Social Services and Public Safety to:
"publish the autism strategy not less than two years after the passing of this Act."
1227. If the Bill is enacted in March 2011, will we be in limbo until 2013? The DHSSPS will have to peddle the Act through a series of groups of civil servants who have to be made aware, first and foremost, of the objective. We have the objective group, and the Bill would stymie everything that we stand for.
1228. Ms White: May I come in to try to come back to what you are asking? I want to give you an example that tries to answer both clauses.
1229. I will give an example of how this affects young people with autism in an education scenario. Cases in which parents are trying to have the educational needs of their autistic young person met often end up at a tribunal or judicial review because of the legislation, which results in high legal costs for the Department of Education, the parents concerned or the health trusts involved. Cases, tribunals or judicial reviews that involve a dispute about the definition of a young person's problem in order to determine how his or her educational needs should be met take away from the ordinary good work of people acting on behalf of that young person in the school and the effective way in which that person's needs are met by their family and school.
1230. An awful lot of time and money are wasted in the education setting today, thereby adding to families' problems and costs all round. We are getting tied up with legislative language rather than working with need on the ground. I know from personal experience and from speaking to many of the parents and families with whom I work on behalf of the South Eastern Trust that whether or not the definition is changed is almost a red herring because the same issues will apply regardless of whether or not the Bill is enacted.
1231. Ken spoke about a strategy being put forward if the Bill is passed. However, there is a strategy right now. It is on the ground and is working. It is working in Belfast and is being emulated, with struggles, in the other trust areas. Nevertheless, it is working and happening. Therefore, we do not need a Bill to put a strategy in place.
1232. Mr Callaghan: At the risk of continuing to get the same answer, it is difficult for us to understand why witnesses — I am not saying that all witnesses do this — say that there is no need for the Bill because it is happening anyway. That raises an inevitable question: why should we not implement the Bill and statutory duties to compel things to happen rather than leave it to the discretion of various Departments or agencies? The Committee will have to address that issue once it has heard all the evidence.
1233. I was interested in something that you said, Nuala. I think that Hansard will show that you said that — this was when we were trying to deal with the DDA, but it is relevant to clauses 2 and 3 — if health, education and others worked in support of the work that is going on, there would be no need for a Bill.
1234. We all accept that there have been improvements. However, the issue is how to maximise future development and maximum delivery for people who need better services. Your statement seems to imply that there is an acceptance that we could do with better co-ordination. Therefore, what is the problem with having a statutory duty to co-operate, which clause 2 states?
1235. Lord Maginnis: From a purely political view — as an elected representative, you will know this —
1236. Mr Callaghan: I was not elected. [Laughter.]
1237. Ms S Ramsey: He was co-opted.
1238. Lord Maginnis: We will not have that diversion.
1239. We have a responsibility. There are things that we should do, and those things that we attempt to do are less constraining than the things that we must do. If the Bill were enacted tomorrow, would you sit on your hands for the rest of your elected time? How do you control, interface and subscribe to the work that we are doing? For example, clause 2(2) states:
"Before preparing the autism strategy, the Department must consult the Northern Ireland departments on it."
1240. How long do you think that it takes — I ask you this question again — to get together groups of civil servants from the 13 Departments? How would you do it? On Saturday, I talked to a Minister — I will not say who it was — who promised to ring-fence a sum of money and to work with part of my group and a new group that will work with and inform his civil servants so that we can create yet another pathway. If I told you that there was a pathway, you would know who the Minister was. Do you know what I mean?
1241. Ms S Ramsey: It has to be the Health Minister because the Minister of Education is female. You said "his". [Laughter.]
1242. Lord Maginnis: Yes. Well, you would not want to distract me with Middletown and such diversions.
1243. Ms S Ramsey: The phrase "poacher becomes gamekeeper" springs to mind.
1244. Lord Maginnis: Clause 2(3) states:
"The Department must request every HSC trust to provide data on the prevalence of autism in its area in order –
(a) that it can publish and update the strategy".
1245. It goes on to give a list of time-consuming nonsense that must be carried out under clause 2. The Bill would take power out of people's hands. It would disempower parents, carers and service users who are fully involved at present.
1246. Mr McCallister: I do not doubt the commitment of anybody in the room to want to help. I agree with Ken that frustration with the service has probably driven much of that. I want to raise a couple of points that the Chairperson and others have put to almost every group from whom we have heard evidence. In your work to date, have you felt inhibited by legislation? Have you hit any barriers? Has anyone said that the law needs to be changed because something does not happen, or is it more a matter of resources?
1247. Ms White: That is a great question. In our experience, whether something is legislated for simply does not come into the picture. We meet the normal resistance of the health and education systems, where an "us and them" history and culture prevails. A medical model is in place. Resistance is met when someone attempts to be an equal player and to have input in his or her family's care or required interventions. That is where inhibitors have arisen. Great movement has taken place on that. Pól's question about whether it will make a positive or negative difference relates to that area. We grapple with exactly that: what difference will it make when work is being done? It feels, genuinely, like a red herring unless a family's only recourse to help is to take the might of the law against the system. There is another way. That reinforces the "us and them" culture. One person might get a result. However, you know better than I do that there is very little money out there, guys. Very little money is available.
1248. Mr McCallister: Earlier today, we heard evidence from the Department of Education. Although it obviously supports the Bill in principle, it is clearly concerned that it could create a hierarchy of conditions and that, rather than targeting need, it would end up targeting autism. I refer to Laura's earlier point about someone having complex needs. Depending on the nature of conditions, can there, in some cases, be great difficulty in identifying how to address need and in determining whether someone gets help? Do you see all those issues coming into play?
1249. Ms White: Absolutely; those issues come into play. What difference will legislation make to that — definition or no definition? I cannot for the life of me see what difference it will make except, perhaps, to set parent against parent. It may, perhaps, exacerbate the "us and them" culture, which we are trying to move away from and towards participation and problem-solving together. For goodness sake; the current London Government are giving out to the UK about changing the way in which we work and community empowerment. Legislation would take us backwards.
1250. Mr McCallister: The Bill states that the DHSSPS will take the lead on the establishment of a cross-departmental strategy. Ken, you mentioned Middletown. I have always used that example, because one could say that the strategies of the Health and Education Departments diverge completely from each other. One says that it is a great idea while the other says that it has severe reservations. I have asked that question of other groups. How would the Health Department, in a lead role, handle that?
1251. Lord Maginnis: As a legislator, I can answer that. You have heard about the different types of autism. You cannot use the Bill, which is hugely flawed, to create a panacea that will cover every Department and meld them together. That will not work. Any Department that finds that it should do something but is prevented from doing so by legislation can amend existing legislation. They can consult, and so on, but that is a practical way to deal with legislation. That has been my experience over the past 28 years.
1252. The Chairperson: Thank you very much, Lord Maginnis, and your team. We are very grateful that you have given evidence on this matter. Particularly towards the end, you certainly hammered home some very strong points from your perspective. That is appreciated.
1253. Dr Deeny: I was going to —
1254. The Chairperson: You did get in earlier.
1255. Dr Deeny: Fair enough.
1256. The Chairperson: The difficulty is that departmental officials are coming at 3.30 pm to brief us on the Budget. It is important that we move on to another very pressing issue.
1257. Ms White: Being a thorn in your side, I beg to raise one more point before we finish.
1258. The Chairperson: Can you do it in one sentence, Ms White?
1259. Ms White: No, I cannot do it in one sentence. I can do it in three sentences. I am a carer; I have a 16-year-old crisis going on in my family, and I have given much of my time to put a case before you. I beg you for the opportunity to add a further significant point.
1260. The Chairperson: Let us be frank: unfortunately, although the end of your submission was very much to the point, some the early part was not relevant at all. That is, unfortunately, why we are short of time. You put some very strong points across when we got to the core issues.
1261. Ms White: I will do it in one sentence.
1262. The Chairperson: Unfortunately, much time was wasted at the start. The other difficulty is that departmental officials are coming to brief us on a crucial issue, which is our £4·3 billion budget for next year. We have to deal with that as well.
1263. Ms White: I will give it in one sentence.
1264. The Chairperson: Put it in writing, Ms White. I guarantee that the entire Committee will get it.
1265. Ms White: OK.
1266. Lord Maginnis: Thank you very much.
27 January 2011
Members present for all or part of the proceedings:
Mr Jim Wells (Chairperson)
Mrs Michelle O'Neill (Deputy Chairperson)
Mr Mickey Brady
Mr Pól Callaghan
Dr Kieran Deeny
Mr Alex Easton
Mr Tommy Gallagher
Mr Sam Gardiner
Mr Paul Girvan
Mr John McCallister
Ms Sue Ramsey
1267. The Chairperson (Mr Wells): We move now to the clause-by-clause consideration of the Autism Bill. I draw members' attention to a letter that has just been received from Dominic Bradley stating that he intends to withdraw clause 3(5). Subsection (5), which deals with training for public/civil servants, will no longer stand part of the Bill. Well done to colleagues who managed to contact Dominic and get that document.
1268. This is the formal stage and is a bit wooden. Those who went through the process for the previous Bills on sunbeds and the safeguarding board will know what to expect. It must be done; it is an essential part of the Committee's duties and is required for the preparation of the Committee report. Therefore, please bear with me as I go through the rather legalistic process. I emphasise that today is the final opportunity for members to propose amendments.
1269. Mr McCallister: It is the final opportunity for the Committee to do so.
1270. The Chairperson: Yes. Individual members may still propose amendments after today. However, as I often say, members have sat through the entire Committee Stage, and I would not like us to be ambushed by late amendments. I will put the Question formally on each clause, and we are required to vote on whether we are: content with the clause as drafted; content with the clause as drafted, subject to the amendment proposed by the sponsor; or not content and wish to amend the clause. Members should note that, if they are proposing a Committee amendment, they must have the text of that amendment with them today.
Clause 1 (Amendment to the Disability Discrimination Act 1995 (c. 50))
1271. The Chairperson: Clause 1 amends the Disability Discrimination Act (DDA) 1995 in two parts, first, through clause 1(2), which amends the definition of disability in the Act. However, Dominic Bradley MLA has tabled an amendment to leave out clause 1(2). Bearing that in mind, clause 1(3) will amend the DDA by extending the definition of the normal day-to-day activities in schedule 1, so that a condition that has a substantial and long-term adverse effect on someone's ability to take part in "normal social interaction" or to form "social relationships" can constitute a disability. Mr Bradley does not propose any amendment to clause 1(3). At the informal stage, the Committee indicated that it was generally content with the clause and Mr Bradley's proposed amendment. This is the last opportunity to discuss clause 1. Does anyone have any concerns?
1272. Mr McCallister: We have concerns and will abstain.
1273. The Chairperson: Do you want that to be noted? Folks, everyone was agreed on the Safeguarding Board Bill, but this is a little more difficult. Do you want to vote formally on each clause? Do you want the vote to be recorded?
1274. Mr Easton: I want a recorded vote, please.
1275. The Chairperson: OK. Are members happy with that?
Members indicated assent.
1276. The Chairperson: OK. We will record each vote.
Question put, That the Committee is content with the clause as drafted, subject to the proposed amendment agreed with the sponsor of the Bill.
The Committee divided: Ayes 6; Noes 0.
AYES
Mr Brady, Mr Callaghan, Mr Easton, Mr Gallagher, Mr Girvan, Mrs O'Neill.
Question accordingly agreed to.
Clause 1, subject to the proposed amendment agreed with the sponsor of the Bill, agreed to.
Clause 2 (Autism strategy)
1277. The Chairperson: Clause 2 requires the Department to prepare and publish a strategy on autism within two years of the passing of the Act and following consultation with other Northern Ireland Departments. All Departments in the Executive are placed under an obligation to implement any part of the strategy for which they are responsible. I remind members that, this morning, you were generally content with the clause. This is the last opportunity to discuss it. Does anyone have any concerns?
1278. Mr McCallister: I have nothing to add to what I said about abstaining.
Question put, That the Committee is content with the clause as drafted.
The Committee divided: Ayes 6; Noes 0.
AYES
Mr Brady, Mr Callaghan, Mr Easton, Mr Gallagher, Mr Girvan, Mrs O'Neill.
Question accordingly agreed to.
Clause 2 agreed to.
Clause 3 (Content of the autism strategy)
1279. The Chairperson: I remind members that the Committee indicated that it was generally content with the clause and the commitment from Mr Bradley to propose an amendment in relation to the term "Civil Service" in clause 3(5). Of course, there is now an amendment to remove clause 3(5). This is the last opportunity to discuss the clause. Does anyone have any concerns?
1280. Mr Girvan: Chair, is it right to say that we are voting on clause 3 with the exclusion of subsection (5)?
1281. The Chairperson: Yes. I will put the Question that the Committee is content with the clause as drafted, subject to the amendment, which is the deletion of clause 3(5), proposed by the sponsor. Take it as read that you would be agreeing to the clause without subsection (5). If you are not happy with Dominic's amendment, you would not vote for the clause.
Question put, That the Committee is content with the clause as drafted, subject to the proposed amendment agreed with the sponsor of the Bill.
The Committee divided: Ayes 7; Noes 0.
AYES
Mr Brady, Mr Callaghan, Mr Easton, Mr Gallagher, Mr Girvan, Mrs O'Neill, Ms S Ramsey.
Question accordingly agreed to.
Clause 3, subject to the proposed amendment agreed with the sponsor of the Bill, agreed to.
Clause 4 (Interpretation)
1282. The Chairperson: This clause defines a number of terms used throughout the Bill. Again, members indicated that they were generally content with the clause. This is your last opportunity to discuss this clause. Does anyone have any concerns? This was not as contentious.
1283. Question put, That the Committee is content with the clause as drafted.
The Committee divided: Ayes 7; Noes 0.
AYES
Mr Brady, Mr Callaghan, Mr Easton, Mr Gallagher, Mr Girvan, Mrs O'Neill, Ms S Ramsey.
Question accordingly agreed to.
Clause 4 agreed to.
Clause 5 (Regulations and orders made under this Act)
1284. The Chairperson: We are getting down to the nitty-gritty of the technical clauses now, folks. This clause contains provision for the required procedures for making subordinate legislation under the Act. Again, members indicated that they were generally content with the clause. This is the last opportunity to discuss the clause. Does anyone have any concerns?
1285. Question put, That the Committee is content with the clause as drafted.
The Committee divided: Ayes 7; Noes 0.
AYES
Mr Brady, Mr Callaghan, Mr Easton, Mr Gallagher, Mr Girvan, Mrs O'Neill, Ms S Ramsey.
Question accordingly agreed to.
Clause 5 agreed to.
1286. Ms S Ramsey: Gerry Adams would fit in nicely with the three of you who are abstaining.
Clause 6 (Commencement)
1287. The Chairperson: This clause provides for the Bill to come into operation three months after the date on which it receives Royal Assent. I know that there is a great deal of enthusiasm for that.
1288. Ms S Ramsey: You never know — the revolution.
1289. The Chairperson: What would the Baron of Northstead say about this?
1290. Mr McCallister: I am sure that he will be able to sign it.
1291. Ms S Ramsey: You would need to ask him, because he received an apology.
1292. The Chairperson: I am sure that he is now up at that level. I remind members that the Committee was generally content with the clause. This is your last opportunity to discuss this clause. Does anyone have any concerns about Her Majesty's signing this off?
1293. Mr Girvan: The Bill might fall on that one.
1294. Mr Callaghan: Chair, just out of curiosity, the draft in front of me states:
"the day on which it was passed."
1295. That is a different text to the one that you read out.
1296. The Chairperson: All Assembly Bills go for Royal Assent.
1297. Mr Callaghan: I accept that.
1298. The Chairperson: You have probably raised an eyebrow or two by saying that.
1299. Mr Callaghan: Rather, I acknowledge that. [Laughter.]
1300. The Chairperson: All Assembly Bills that I have dealt with include that phrase. I know that that phrase causes a difficulty for some people, and I understand what you are trying to say, but it is included each and every time. Therefore, we just have to accept it.
1301. Mr Brady: Can we put down a question for urgent oral answer asking whether The Queen does, in fact, read all these Bills?
1302. The Chairperson: I am certain that she will read the Bill and the Assembly report.
1303. Mr Brady: I will take your word for it.
1304. Ms S Ramsey: She will read them in between watching 'Shameless'.
1305. The Chairperson: Let us return to some sense of seriousness, because it is a very serious issue. It is entirely my fault that this meeting has gone downhill.
1306. Question put, That the Committee is content with the clause as drafted.
The Committee divided: Ayes 7; Noes 0.
AYES
Mr Brady, Mr Callaghan, Mr Easton, Mr Gallagher, Mr Girvan, Mrs O'Neill, Ms S Ramsey.
Question accordingly agreed to.
Clause 6 agreed to.
1307. The Chairperson: That is our knighthoods down the drain.
Clause 7 (Short title)
1308. The Chairperson: This clause provides for the short title of the Bill. Again, there was absolutely no concern, apart from the one issue about the date, but I am sure that that will be sorted out. I remind members that they indicated that they were generally content with the clause.
1309. Question put, That the Committee is content with the clause as drafted.
The Committee divided: Ayes 7; Noes 0.
AYES
Mr Brady, Mr Callaghan, Mr Easton, Mr Gallagher, Mr Girvan, Mrs O'Neill, Ms S Ramsey.
Question accordingly agreed to.
Clause 7 agreed to.
Long title
1310. The Chairperson: Again, there were no issues with this.
1311. Question put, That the Committee is content with the long title of the Bill as drafted.
The Committee divided: Ayes 7; Noes 0.
AYES
Mr Brady, Mr Callaghan, Mr Easton, Mr Gallagher, Mr Girvan, Mrs O'Neill, Ms S Ramsey.
Question accordingly agreed to.
Long title agreed to.
1312. The Chairperson: Kieran, we are not sure how you voted on the long title. You voted for the short title, but we do not know how you voted on the long title. There is, obviously, a deep split in the Kieran Deeny party.
1313. Dr Deeny: I am sorry. I just came in late, and I am not really up to speed.
1314. The Chairperson: In that case, it would be better to join with those who abstained.
1315. Dr Deeny: On both?
1316. The Chairperson: Yes. It will not make any difference. That, folks, is the end of this stage of the deliberation on the Bill. There will be a Committee report, and the further stages will take place on the Floor of the House. Thank you for your help.
Appendix 3
Written Submissions
Contents
1. Autism NI
2. Northern Ireland Human Rights Commission
3. College of Occupational Therapists
4. Parent Carers' Council on Disability
8. Parents' Education as Autism Therapists (PEAT)
9. Department for Regional Development
10. South Eastern Education and Library Board
11. Belfast Education and Library Board
12. Southern Health and Social Care Trust
13. Southern and Western Education and Library Boards
16. North Eastern Education and Library Board
17. Carers NI
18. Royal College of Speech and Language Therapists
19. South Eastern Health and Social Care Trust
20. Mencap
21. Royal College of General Practitioners
22. Northern Health and Social Care Trust
24. Department of Enterprise, Trade and Investment
26. Department of Finance and Personnel
27. Belfast Health and Social Care Trust
28. Regional Autistic Spectrum Disorder Reference Group
30. Department of Health, Social Services and Public Safety
31. Department of the Environment
32. Office of the First Minister and deputy First Minister
Autism NI
Autism NI Credentials
Length of service to the ASD Community in Northern Ireland (NI).
The Charity celebrated its 20th anniversary this year (2010). It was established in 1990 as NI's indigenous Autism charity.
In 1992, only six children in NI had a diagnosis of ASD. In 1992, the Library Service only had one title on ASD, so Autism NI donated supplies of the second title.
N.B. Autism NI (PAPA) – the only NI ASD charity to be regularly evaluated over 20 years.
Mandate
Autism NI supports a network of over 30 groups and Branches across NI involved in local activities and run by local families living with ASD. Each group supports between 10 and 100 families at a range of events.
Autism NI also has a membership base currently totalling over 800 families and agencies.
The charity also supports an active Parent lobby for improved services and required legislation (PAL). PAL is run by parents for parents. It is the parent political voice of the charity.
Research
Autism NI has created the largest portfolio of NI research on ASD across the Voluntary and Statutory sectors on issues ranging from specific interventions (such as TEACCH and social skills models) to cross agency early intervention models and programmes (Keyhole® Programme) as well as Training (DHSSPS ASD Training Strategy for ASD 2006), Diagnosis of ASD and Family Support ("Hidden Community" and "Is anyone Listening"). The Research partnership with UU has involved Education.
Advocacy and Awareness of ASD
Building upon the above Research portfolio, Autism NI has combined its training and family support functions to create awareness of ASD.
April has been established as Autism Awareness Month and further strengthened by the UN designation of April 2nd as World Autism Awareness Day.
Media/press contacts and relationships have been established and this was extended to our regional groups from 2005 with specialised media and lobby training. From this exercise in participative parent empowerment a Policy Committee emerged which evolved into the Parent Autism Lobby (PAL).
Training
Autism NI has brought world experts to NI and been responsible for many "firsts", e.g. first PECS training in Ireland, first Diagnostic (ASD) training.
2004 – Autism NI Regional ASD Training Department (established and funded by DHSSPS).
2006 – NI ASD Training Cross Departmental Strategy (UUJ) (funded by DHSSPS).
N.B. Achievements:-
Autism NI is an Accredited Examination Centre (AQA)
Autism NI provides the only accredited ASD courses outside NI Universities.
Autism NI co-founded the UU web based ASD module.
Autism NI has trained 4,000 – 6,000 delegates annually.
Autism NI has had its training function independently evaluated and audited.
Innovative packages for all sectors, e.g. Justice System.
Family Support.
Developed from membership and Branch mandate.
Specialised Family Support training (for siblings, grandparents and fathers).
Family Support service model – commissioned across three HSCTs.
Helpline.
Strategic Development Role.
The only ASD Charity in NI to be regularly evaluated over 20 years.
Partnership across sectors (15 Voluntary partners and Statutory Sector).
The ASD Diagnosticians Forum (Founder Member).
ASD strategies within HSCTs (Autism NI initiation, lobby role and involvement).
DENI Task Group report (Autism NI was Steering Group member).
Bamford Review (Autism NI exposed flawed recommendations re ASD).
DHSSPS Action Plan
The Autism Bill (NI)
Celtic Nations Autism Partnership (and Atlantic Autism Alliance).
All Party Group on Autism.
Challenges for the future.
ASD Budget
ASD Policy
RPA
Role of the Voluntary Sector.
The Autism Bill (NI)..............expanded below.
NEED?
HUMAN AND FINANCIAL COST.
EQUALITY?
IMPACT FOR FAMILIES FROM THIS BILL.
DHSSPS ACTION PLAN & DENI FRAMEWORK.
IMPLEMENTATION OF THE AUTISM ACT (HOW?).
AMENDMENTS? E.G. ADVOCATE ROLE, "PUBLIC SERVANTS".
THE PARENT AUTISM LOBBY (DAVID HEATLEY, CHAIRPERSON).
A PRINCIPLED STAND BY AUTISM NI – THE COST.
NEED?
I can quote you figures from recent research carried out by the Voluntary Sector .....
80% of mothers experiencing high levels of anxiety through to 50% who are on long term anti depressant medication.
64% of adults with ASD live at home, 13% live on their own, and 25% are financially independent.
57% of adults with ASD have suffered depression, 65% anxiety and 34% mental health problems as a result of lack of support.
I can quote you prevalence figures from DENI....
5000 school age children with ASD (900 in 2002)
suspected prevalence rise of 1:100 to 1:60 within the past 3 yrs.
I can quote you targets set by DHSSPS regarding waiting lists for diagnosis.
I can remind you of the recent Judicial Decision regarding ASD services failures.
I can reference to the Committee the AutismNI Report cataloguing the hours spent on ASD statutory service reviews and strategies even prior to the current DHSSPS and DENI work.
I can reference to the Committee the DHSSPS funded University of Ulster report "An ASD Training Strategy for NI" written prior to the yearlong deliberations of the DHSSPS Action Plan on the self same topic.
I can encourage the Committee to consider the NI Assembly Research and Library Service reports on the pros and cons of strategies versus legislation in the NI context.
BUT....the conclusion remains the same! There has been more talk than effective action.
Prevalence rates increase by 500% and funding increases by 100%
HUMAN AND FINANCIAL COST.
I can quote you the work carried out in Australia, Canada and UK regarding the costs to the State of mishandling the issue of ASD set against the backdrop of the cost effectiveness of intensive early intervention and family support.
I can reference to the Committee the analysis completed by AutismNI - "Autism: The Costs"
But the reality remains - The cost of ineffective leadership and engagement on the issue of ASD in Northern Ireland is incalculable and shameful.
Wales, by comparison, has been 'ASD informed' and systematic and professional.....building upon existing expertise and not throwing the baby out with the bathwater and reinventing the wheel as we are in Northern Ireland under the cloak of service redesign.
All this means is pushing clinicians to rush through increasing numbers of diagnoses to meet targets adopted from Hospital environments (trolley waits etc)...and the result for ASD is incomplete or recycled or delayed assessments as quality of contact and diagnosis suffers.
We will address the human cost through the presentation of one single case story and if the Committee wishes we can elaborate on the detail in members questions afterwards......this is one of many that lie behind the statistics referenced earlier.......Finn case study!!! (submitted to Alex Easton MLA, Acting Chairperson)
EQUALITY?
In addition to the APGA consultation and contact with the ECNI and Disability Action, I met this week with Brice Dixon and representatives from the NIHRC to progress mutual understanding on the purpose and need for the Bill to address the issue of equality for ASD within disability law. [The NIHRC questioned the selection of DHSSPS as the lead department in view of the need for all such legislation to be synchronised with the UN Convention on Disability under OFMDFM].
The UK/ROI –
DDA repealed and Equality Act introduced, definition of disability in ROI includes "sensory".
N. Ireland debating still –
The Bill of Rights (NI)
Northern Ireland compliance with the UN Convention on the Rights of Persons with Disabilities.
The above developments will impact on ASD if ASD is "at the table"
The Autism Act (NI) will guarantee that ASD has a seat at the table.
Meanwhile, the DDA is the only show in town and it doesn't include ASD per se. It needs to be updated to take account of the changing world of disability as a greater proportion of our population are being diagnosed with ASD. Remember please, that in 1995 when the DDA was introduced, we had a couple of dozen children formally diagnosed with ASD, no training in diagnostic techniques and tools and only one or two professionals committed to the need for diagnosis.
So let's make a difference now. Why wait when we can make practical changes now to make services and benefits more accessible and less of a fight for families.
IMPACT FOR FAMILIES FROM THIS BILL.
DLA guidance use DDA definition of disability.
DSD regulations regarding housing adaptations (physical markers dominate).
DE discipline codes need to recognise "ASD behaviours".
ASD Awareness for public and ASD training for public servants....e.g.Finn case study!! (submitted to Alex Easton MLA, Acting Chairperson)
ASD Service planning across departments and transitions.
Emotion impact of recognition.
DHSSPS ACTION PLAN & DENI FRAMEWORK.
Limited by lack of "buy in" from other departments.
DHSSPS ASD Strategy relies on medical not social model so balance of resources have gone to diagnosis not early intervention or family support.
DENI ASD Framework does not include an operational partnership role for the voluntary sector.
DHSSPS engagement model with non mandated carers and individuals with ASD is reckless....unsupported and unresourced.
IMPLEMENTATION OF THE AUTISM ACT (HOW?).
Leadership is crucial.
Respect is essential.
Secondment from Wales (MOU).
THE PARENT AUTISM LOBBY (DAVID HEATLEY, CHAIRPERSON).
I will shortly hand over briefly to David Heatley who will present his own perspective on the Autism Bill with evidence from the PAL parent mandate from across Northern Ireland.
A PRINCIPLED STAND BY AUTISM NI – THE COST?
AutismNI has remained constant to its political lobby dating back to 2001 and to its pledge in 2006 to campaign for ring fenced funding, a cross department strategy and legislative recognition for ASD.
Since 2008, AutismNI has been subject to threatened investigations and withdrawal of DHSSPS, Regional Board and HSCT funding as well as expulsion from the RASDN Reference Group – unless it "parked legislation".
In 2010, those threats were directed personally towards the CEO and Director of Development.
In 2010, AutismNI won recognition of its principled, dignified and professional stand for social change from the Voluntary Sector when presented with the CO3 Voyager Leadership award in Political Impact.
AutismNI may pay the ultimate price for this principled stand unless this position is reversed and relationships are actively reconstructed.
Submisssion by AutismNI (16.12.10).
Parents Autism Lobby
The Parents Autism Lobby is the parents voice from within the charity. We represent 30 groups across Northern Ireland, the list is on the sheet provided.
These Branches vary from perhaps ten members to much larger groups of over fifty members, a few have over one hundred members affiliated to them.
AutismNI has approx. 800 registered families(+agencies)who are members of the charity, but all branches also have families that have not formally "joined" the charity, but who would count themselves as members of the local group.
Therefore I can quite confidently say that PAL represents over 1000 families across Northern Ireland.
This mandate gives me confidence in backing every statement that Autism NI has made at this presentation.
I have been in very regular contact with the Branch/Support Group Network by phone and by letter.
I have personally visited almost half of the groups in person over the past nine months and have meetings set up for another five by the first week in February. In all my contacts I have had no parent, not one who thinks we would be better off without legislation.
So what do I hear:
Why has it taken so long?
Is it not just common sense?
We need joined up government
Services are terrible!
After diagnosis no one was there to help or explain!
Everyone is too busy to help me, I'm on my own!
Unless you live with Autism you can't possibly understand!
The branches I have mentioned before vary from some that are totally new and still being set up, to some branches that have been established for many years. The expertise within these branches is only surpassed by the expertise and professionalism of the AutismNI Staff Team, many of whom are also parents of individuals with ASD.
The very first Diagnostic Training in Northern Ireland took place in 1997. That training was set in place by AutismNI and was funded by the East Antrim Branch. Since then there has been training every year, thanks to AutismNI. In recognition of this, AutismNI was made an honourary member of the independent NI Autism Diagnosticans Forum, a grouping of ASD experts unique within the UK and Ireland. Most Diagnosticians and other experts in Autism within Northern Ireland have received much of their training through the charity.
Parents are very angry that the twenty years of work, expertise and partnerships that is AutismNI has been to a large extent overlooked in the past year and a half.
The AutismNI Lobby started in 2001.
AutismNI is a founder member of the Celtic Nations Autism Partnership and the Atlantic Autism Alliance.
In 2006 Northern Ireland was ahead of Wales in its aim for a National Autism Strategy…but politics got in the way.
Our parents, sadly, are used to being let down. So much has been promised in the past, seeds were sown, but the fruit never ripened, it withered on the vine.
Please make sure that this is not another blind alley.
The Autism Community desperately need this bill.
They are disadvantaged by a disability that is not recognised in law
Parents are already under unbelievable stress because of the very nature of the condition, and not only the parents but the siblings, the grandparents, the wider family circle, the carers and the schools.
This Bill needs to "Do What it says on the Tin" it needs to be strong and watertight. It needs to go through…
…If however it fails
…we will be back,
…we will not let it rest,
…we will lobby, lobby, lobby because we are so sure that it is the only way forward that can ensure equality for ASD.
Ballycastle Support Group: Ballycastle
Ballymena Support Group: Ballymena
Ballynahinch & Dromara Support Group: Ballynahinch
Brookfield Support Group: Moira
Castlederg Branch: Castlederg
Clifden Support Group: Bangor
Craigavon & Banbridge Support Group: Lurgan
Crumlin & Glenavy Branch: Crumlin
Down Branch: Dundrum
Dungannon & Armagh: Dungannon
East Antrim Branch: Ballyclare
Fermanagh Branch: Enniskillen
Helping Hands Affiliated Group: East Belfast
Holywood Support Group: Holywood
Lisburn Branch: Lisburn
Mid-Ulster Branch: Maghera
Newry & Mourne Branch: Warrenpoint
North Coast Branch: Coleraine
North Down & Ards Support Group : Newtownards
North West Branch: Londonderry/Derry
Omagh Support Group: Omagh
Peninsula Support Group: Kircubbin
Strabane Support Group: Strabane
South Belfast Branch: Knockbracken
South Down Branch: Newry
Tor Bank Partnership Group: Dundonald
West Belfast Support Groups (4):
Ballyowen Health Centre, Anderstown
Holy Child School, Anderstown
Good Shepherd Nursery, Poleglass
St Paul's School, West Belfast
Autism NI position on the Autism Bill (NI) 2011
- Clause 1. - Autism NI supports the changes to the DDA. The inclusion of social and communication impairments in the definition of disability is a long overdue update to existing legislation and it will secure recognition of ASD and implement measures to achieve improved access to services, statutory benefits and public facilities.
AutismNI views the current "mental and physical" definition of disability to be discriminatory against ASD.
- Clause 2. – Autism NI supports the critical need for a cross department ASD strategy to establish lifelong service plans that ameliorate the particular challenges experienced by individuals with ASD across life transitions.
Autism NI is also mindful of the need to consult with, integrate and recognise the contribution of the Voluntary Sector and families they represent and assumes that as this is accepted best practice, this principal will be automatically integrated within any strategy in an efficient and time effective model.
- Clause 2(2) and 2(7) and (8) – Autism NI views this legal requirement on all departments to plan and implement the ASD strategy as an injection of much needed accountability and transparency into ASD planning and provision by government. Failure to comply becomes a matter for the Northern Ireland Executive to address.
- Clause 2(3) and (4) – Autism NI supports this measure and is mindful that DENI has been the lead agency in ASD data collection with more recent steps being planned by DHSSPS and therefore applauds the provision within the Bill for cross departmental data synchronisation as the basis for future planning across life transitions.
- Clause 2(5) and (6) and (9) and (10) – Autism NI supports the monitoring network outlined within these clauses that will provide the NI Assembly with the necessary information, access and mechanism to analyse and assess the need to introduce the currently deferred role of the Autism Advocate to arbitrate, investigate and advocate for individuals with ASD and their families. Autism NI regrets the omission of the role of an Autism Advocate to secure progress, consistency, effective structure and much needed respected leadership but respects the need to limit additionality in the current economic climate if possible.
- Clause 3(1) – Autism NI commends the recognition of the lifelong nature of ASD and interprets this clause as the commitment to the critical cross departmental planning process across life transitions.
- Clause 3 (2) – Autism NI is appreciative of the Bill's prioritisation of the areas detailed to further clarify the more general clause above and to remind us of the need for placement of support services in the home, school and community. Furthermore Autism NI would be concerned about the critical gap regarding recognition of the overwhelming evidence that supports the effectiveness of early years intervention. Autism NI therefore puts on record, for the Bill implementation stage, the critical relevance of international and local research on the pivotal importance of quality accredited intensive early intervention practice models such as those profiled by Autism NI (Keyhole®), PEAT, SPEAC and CEAT.
- Clause 3(3) – Autism NI, founded upon the principals of community development, family support and empowerment, commends the Bill in drawing out legislative recognition of the support needs of families living with ASD.
- Clause 3(4) - Autism NI welcomes this legislative support for a government ASD awareness campaign across the community. Autism NI has over the past 20yrs led this critical work within existing resources, having established campaigns to build upon Autism Awareness Month (April) embracing the Cuppa-Aid events and the UN designated World Autism Awareness Day (April 2nd). Autism NI would welcome the opportunity to provide continuity and reduced duplication through the lead role in the continued evolution of this work.
- Clause 3(5) – Autism NI supports the need for a cross departmental training strategy as part of the strategy required under this legislation and therefore supports this clause. It is to be hoped however that this clause, requiring ASD training for civil servants, would fall within that remit. Autism NI would welcome consideration over the change from 'civil servants' to 'public servants' under the rationale that there are various levels of awareness and targeted training needed across all sectors likely to be in contact (to varying degrees) with people with ASD
- Clause 3 (6) –Autism NI recognises the lead role of the DHSSPS within the planned legislation and reinforced within this clause.
Summary comments:
Autism NI's relationship with the DHSSPS has suffered over the last two years as a direct result of a divergence of opinion regarding the role of legislation for ASD. Autism NI would welcome proactive intervention from the Minister of Health, Social Care and Public Safety in June 2011 to restore a positive working relationship and a recognised role for Autism NI in view of previous threats to funding and participation.
Autism NI would also welcome consideration by the Minister of Health, Social Care and Public Safety, of a Memorandum of Understanding with the Welsh Assembly Government in view of the Welsh experience in implementing a cross departmental mechanism for ASD. This would secure the required partnership assistance towards establishing effective implementation structures especially in the oversight of joined up and planned services across the transitions. Within this, a secondment of the current Wales ASD implementation officer would be an advantage.
NB. Autism NI is proud to be associated with the Autism Bill (NI) and is hugely grateful to Dominic Bradley, the APGA members and all the MLAs who have listened studied and acted.
Northern Ireland Human Rights Commission
1. The Northern Ireland Human Rights Commission (the Commission) is a statutory body created by the Northern Ireland Act 1998. It has a range of functions including reviewing the adequacy and effectiveness of Northern Ireland law and practice relating to the protection of human rights[1], and advising on whether a Bill is compatible with human rights.[2] In all of that work, the Commission bases its positions on the full range of internationally accepted human rights standards, including the European Convention on Human Rights (ECHR), other treaty obligations in the Council of Europe and United Nations systems, and the non-binding 'soft law' standards developed by the human rights bodies.
2. The Commission welcomes the opportunity to comment on the provisions in the Autism Bill introduced by Mr Dominic Bradley MLA. We base our comments on the United Nations Convention on the Rights of Persons with Disability (CRPD) which was ratified by the United Kingdom on 9 June 2009. The Human Rights Commission is designated, along with the Equality Commission for Northern Ireland, the Scottish Human Rights Commission and the Equality and Human Rights Commission, as part of the Independent Mechanism required under CRPD to protect, promote and monitor implementation of the CRPD, but the present submission is made by the NIHRC alone.
3. The Commission supports the intention in clause 1 to amend the Disability Discrimination Act 1995 (DDA), as it applies in Northern Ireland, to include social and communication impairments within the definition of disability. As the state has endorsed the CRPD's use of the social model of disability, the statutory definition should also reflect this position. The DDA as enacted reflected the medical model that is wholly out of step with current thinking on disability. The Commission would prefer to see a fuller incorporation into the DDA of the wording from Article 1 CRPD, the second sentence of which reads:
Persons with disabilities include those who have long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others.
4. Such a definition clearly encompasses autistic spectrum disorders (ASD). In the interests of parity of access to rights, there is a case for seeking to amend s.1 and Schedule 1 of DDA (pending new equality legislation in Northern Ireland) and relevant provisions in the Equality Act 2010 (which applies in Great Britain) to directly reflect CRPD concepts on a UK-wide basis. However, as the present Bill only addresses the DDA's application in Northern Ireland we are unclear as to why it does not simply seek to amend Schedule 8 (which deals with modifications of the DDA in its application to Northern Ireland). Whether or not the Autism Bill progresses, the Commission will continue to advocate revision of disability and equality law to bring it fully in line with the CRPD.
5. The Bill goes on to propose that an Autism Strategy, of a specific scope and following a particular methodology, be required by law. The Commission does not view so specific an approach as a requirement of CRPD or any international human rights instrument, and is aware of concerns that legislation seeking to address the needs of one group of persons with disabilities could delay, or divert attention and resources from, the coherent, consistent, comprehensive and proportionate response that is required to ensure equal recognition of and protection for the human rights of all disabled people.
6. However, the Commission is also aware that the needs of persons with autistic spectrum disorders have not been well served to date. It accepts that there is a need for inter-departmental co-ordination to ensure that, for example, health, social services, education and social security provision work together to ensure that needs are assessed and addressed in an effective and timely manner, particularly at key transition points in the lives of persons with autism. A strategic approach such as the Bill envisages would have significant practical benefits, for example in terms of adaptations to public spaces and facilities (with consequential benefits for persons with other disabilities), and recognition of ASD in law would assist decision-making on benefit entitlement. An inter-Departmental strategy would diminish the likelihood of different criteria for access to services being applied across the Trusts, and would raise public awareness and understanding of ASD. It is already apparent that, in the Committee and on the floor, the Bill has raised awareness and understanding among legislators on a cross-party basis, and that achievement will stand whatever the fate of the measure itself.
7. The Commission would prefer to see the introduction by Government of a national disability action plan that would endeavour to realise the full implementation of CRPD for all disabled people. While this could take the form of a UK-wide plan, presumably co-ordinated through the Office for Disability Issues which is designated as the central government 'focal point' for CRPD purposes (Article 33(1) CRPD), in the absence of any state-wide initiative the Northern Ireland Executive could devise a regional strategy or action plan dealing with all matters that are devolved.
8. The Bill proposes that an interdepartmental autism strategy be entrusted to the Department for Health, Social Services and Public Safety (DHSSPS) as the lead. The Commission is concerned that locating the lead role in DHSSPS risks reinforcing the misconception of autism, and of disability more generally, as a medical issue. It is also well established that the DHSSPS is not at present persuaded of the need for the present Bill, so that, should it be enacted, the Department – while it would be bound to implement what is required of it – might not prove to be the most enthusiastic champion of the expected approach.
9. The Commission notes that the Office of the First Minister and deputy First Minister (OFMdFM) has been designated as the CRPD 'focal point' for Northern Ireland. This requires OFMdFM to spearhead a cross-Departmental approach to oversee the implementation of the Convention. Each Department is required to meet the human rights and equality obligations set down by the Convention. These include the full range of civil, political, economic, social and cultural rights, which apply equally to disabled people. Article 31 of CRPD requires the state to collect appropriate information, including statistical and research data, to enable it to formulate and implement policies to give effect to the Convention. Overall, many of the elements included in the Autism Bill are covered by the obligations deriving from CRPD which the state has ratified and is now obliged to deliver.
10. The needs of persons with autism would not be best served by, on the one hand, OFMdFM leading on a comprehensive CRPD-based disability strategy and DHSSPS at the same time leading on a bespoke strategy for autism. The dangers of duplication, conflict, competition for resources and delays in co-ordinating approaches are self-evident. The potential for overlap and conflict is already apparent in relation to autism, where the Education and Health Departments are pursuing separate plans, while other Departments with relevant functions have no plans. The Commission therefore recommends that, should the Autism Bill progress, consideration be given to designating OFMdFM as the lead so that the strategy on ASD can be woven into the anticipated CRPD implementation strategy.
11. The Commission would also make the point that a strategy does not actually require to be set out in legislation, and it may even be that a more efficient, responsive and dynamic approach can be taken without statute. The Welsh Government has adopted and is implementing what autism organisations regard as a highly effective Action Plan for ASD; Scotland recently decided to adopt a cross-departmental ASD strategy; in Denmark, the National Autism Plan is the product of co-operation between approximately 50 Danish experts on autism, an expert committee and an editorial group, and other jurisdictions have strategies or plans that are not based in law. In England, where the Autism Act 2009 mandated production of a strategy, the lead role was given to the Department of Health (whereas CRPD matters are led by the Office for Disability Issues) and guidance on the strategy's implementation is still awaited as of December 2010. It is entirely possible to devise and implement a strategy without setting out its parameters and processes in statute as the Bill seeks to do. Northern Ireland has ready access to expert advice from, for example, the Welsh administration, which we understand has indicated its willingness to share best practice.
12. The Commission underlines that the purpose of CRPD (as noted in Article 1) is to 'promote, protect and ensure the full and equal enjoyment of all human rights and fundamental freedoms by all persons with disabilities'. The Convention makes repeated reference to the realisation of human rights 'on an equal basis with others'. This refers to equality between, and among, non-disabled and disabled people. In that context, the Commission does not consider that special legislation for the rights and needs of people falling within a particular spectrum of disorders is consistent with the equality principle in CRPD.
13. If the Northern Ireland Executive and each of its Departments implemented the CRPD there would be no necessity for an Autism Bill or comparable single-issue Bills. The effective implementation of the Convention requires revision of the DDA to reflect the social model of disability as endorsed by the CRPD.
[1] Northern Ireland Act 1998, s.69(1).
[2] As above, s.69(4).
The College of Occupational Therapists
Introduction
The College of Occupational Therapists (COT) is pleased to provide a submission to the Committee for Health, Social services and Public Safety about the proposed Autism Bill. The College of Occupational Therapists is the professional body for occupational therapists and represents over 28,000 occupational therapists, support workers and students from across the United Kingdom. Occupational therapists work in the NHS, Local Authority social care services, housing, schools, prisons, voluntary and independent sectors, and vocational and employment rehabilitation services.
Occupational therapists are regulated by the Health Professions Council, and work with people of all ages with a wide range of occupational problems resulting from physical, mental, social or developmental difficulties.
The philosophy of occupational therapy is founded on the concept that occupation is essential to human existence and good health and wellbeing. Occupation includes all the things that people do or participate in. For example, caring for themselves and others, working, learning, playing and interacting with others. Being deprived of or having limited access to occupation can affect physical and psychological health.
Amendment to the Disability Discrimination Act 1995
The COT would like to clarify that the proposed route for introducing the Bill via an amendment to current legislation has been based on what is best for people with autism rather than what may be the easiest method of introduction for the Department.
Autism strategy
The COT is in agreement about the need to prepare a strategy on autism that will be fully consulted on. This consultation should include all stakeholder groups who will be involved in the delivery and monitoring of the strategy including professional groups, individuals with autism, families and carers. The COT supports the idea that every HSC trust must provide data on the prevalence of autism in its area and that progress towards the strategy should be reported on every three years by the Department.
Content of the autism strategy
The COT would like confirmation that this strategy is intended to cover adults only. The COT would also like to check that the proposed needs that will be covered such as the "health, educational and social needs of persons with autism" will also include the following:
- The key occupational areas of people with autism's lives: self care activities including the ability to look after oneself and home, employment activities or the main productive role by which one contributes to society and leisure activities. This type of assessment can be carried out by occupational therapists. Occupational therapists can also assess the need for suitable living environments which would involve an assessment of the person's occupational performance (what the person can do), desired goals and communication needs.
- An in-depth, specific sensory assessment carried out by an occupational therapist. A sensory assessment will include asking questions about how the person reacts to sound (e.g. do they stay away from noisy settings), smell (e.g. do they particularly like strong smells like washing powder), taste (e.g. do they particularly like/dislike strong tastes), sight (e.g. do they prefer the curtains closed on a sunny day), movement (e.g. do they like swaying or rocking) and touch (e.g. do they twist their own hair). This information often helps family members or support staff learn how to adjust the environment to facilitate an individual's goal orientated activity.
We would therefore like to suggest the additional wording of "Without prejudice to the generality of subsection (1) the needs to be set out in the autism strategy shall include the health care, occupational, sensory, educational and social needs of persons with autism".
The COT believe that this autism strategy should aim to enable people with autism to have a socially included, ordinary life with access to the same opportunities that most people take for granted such as a home of one's own, relationships, employment and leisure time.
The Parent Carers' Council on Disability
The Parent Carers' Council on Disability was established in 2005. This Council came about from a number of parents with children and young people with disabilities. As parents we did not make a difference in what the child's disability was for e.g. if it was learning disability, physical disability or sensory disability or a prolonged condition which impacted on daily living. As a group of parents we felt we were the experts in our child and young person's life. Our vision was to seek new and distinctive ways of working with the different multi-agencies and professionals that came into contact with the lives of our children and young people. We wanted to make a difference to the lives of children with disabilities and their families. We also wanted to have our own voice as we felt we were let down by the volunteering and statutory agencies. We, as a group, felt that the best people to plan for their child and young person is their parent/carer as we have first hand experience of our child's condition.
Our families go through a grieving process. We go through stages of denial, shock, anger, guilt, overwhelming anxiety, sadness and even depression before we are able to accept the reality of our child's disability – this is a continuous process.
The Parent Carers' Council on Disability is involved in:-
- Regional ASD Work.
- Looked after Children (LAC).
- Northern Ireland Social Care Council
- Regulation & Quality Improvement Authority
- Social Care Institute for Excellence
- Carers' Reference Group (Southern Trust)
- Wraparound & Children's Services Planning
- Training
- Department of Health Social Services & Public Safety
- Health & Social Care Board
- Public Health Agency Health & Social Services
- Education & Library Board
- Guidelines & Audit Implementation Network (Adults with a Learning Disability in Hospital)
- Patient Client Council
- Department of Health & Social Security (DLA Branch, Castle Court, Belfast)
As you can see from the above our involvement is expansive. As parents we feel it is important to be involved in the planning and development of services. This is only a small part of the work carried out by the Parent Carers' Council on Disability. If you would like more information please do not hesitate to contact Mrs Mary Duffin, Chairperson.
The 1995 Disability Discrimination Act (DDA) defines disability as a "physical or mental impairment which has a substantial and long term adverse effect on a person's ability to carry out normal day to day activities". This is the legal definition of disability and is applicable to all public bodies. It is the opinion of the Parent Carers' Council on Disability that this Act covers both Autism and Aspergers.
The Parent Carers' Council on Disability would like to know:-
- What does the Autism Bill offer to families on the ground on a daily basis that we have not already got?
- Will the Bill provide a better quality of services for families for e.g. respite, speech & language, occupational therapists, better schooling?
- Will there be better support for families?
- Will there be better access to services?
- How many other Autism Groups were spoken to?
- How many other disability groups views were sought?
- How much is this Bill going to cost and at what cost to existing families in the disability world?
The Parent Carers' Council on Disability welcomed the Regional Autism Spectrum Disorder Network (RASDN). As a Council we also support the work to date that RASDN has done. We are delighted that parents and service users are involved in this work. We as a Council feel that not all the members of the Health Committee have read all the information and material on RASDN. Had they done so they would not be supporting for another Autism Strategy. Given the current economical climate we feel that at this moment in time it would be a waste of resources which could be spent to help and provide services for all families with disabilities. Parents have raised concerns about dual diagnosis and do not understand how a Bill could help them. Some of these families have children and young people with Down Syndrome, Epilepsy, Cerebral Palsy and Mental Health problems, Autism is not the primary diagnosis but the Autism has a major effect on their lives. What does the Bill entail for these families? Would it not be better if we had a Bill for all disability instead of putting our children and young people into silos? A child or young person should be seen first as a person and their diagnosis second. If there was more Person Centred Planning, more working together, families would feel much better and more equipped to deal with their everyday situation. We also feel that if voluntaries would work more together and listen to families, life for families would be much better. We would also like to remind you that one size does not fit all. When you look at Autism from beginning to end it is a very long, diverse journey. No two children/young person with Autism are the same so we think it is time that we all work together in the good and the better for the children and young people. We would also like to see the end of the internal battles in the ASD world as it is not good for families.
As a Council we feel the way forward is working in partnership, providing information, giving families choices, equality and to be involved in the planning and decision making of their child/young person's life. We as a Council will continue with this ethos. We hope that you will now have a better insight and understanding of the emotional rollercoaster of life that we are on.
On behalf of the Parent Carers' Council on Disability we would like to thank you for giving us this opportunity to express our thoughts on this Bill.
Parent's Autism Lobby
PAL would like to briefly give written evidence to the bill.
Section 1:
Amendment to the Disability Discrimination Act 1995 (c. 50)
PAL acknowledges that within DHSSPS, generally Autism is recognised as a disability (under the mental health or learning disability budgets) and that services are provided on a needs basis not a diagnosis basis. However the needs of individuals with Autism are much wider than DHSSPS's remit and other government departments do use the descriptions within DDA to allocate resources and provide funding.
Currently individuals have difficulty accessing DLA because Autism is not listed in the DDA
Section 2:
The Autism Strategy
PAL recognises that DHSSPS has an Autism Strategy and that DENI are working towards an Autism Strategy, however Northern Ireland needs a Cross-Departmental Autism Strategy such as in place in Wales because Autism Needs implicate on many government departments.
Currently there is a lack of coordination between departments so that there is duplication of some aspects, and gaps in other services. Training is patchy and parents and individuals have to fight for recognition repeatedly, rather than the diagnosis being made and information shared between departments to allow a simple system for individuals with Autism (which by diagnosis recognises communication difficulties). Currently individuals with Autism (or their parents) are having to deal with each department in isolation.
Section 3:
Content of the Autism Strategy
PAL recognises that DHSSPS has made progress in reducing waiting lists for initial diagnosis. A holistic approach is needed however, looking at cradle to grave services for this life-long condition. Quality diagnosis should be followed by early intervention and a package of support provided for the family. Additional resources should be ready for those who need them particularly at periods of transition. Supported employment and supported housing should be available when required. Autism related questions should be on the DLA form, many of the issues faced by individuals with ASD and their families are ignored in the form and questions on the form are irrelevant to them. The Department of Policing and Justice should be aware of the risks individuals with ASD have of being misinterpreted by the system and have systems in place for interviewing individuals with ASD in a suitable environment with advocates to support their difficulties in communication skills.
The current situation is that many report cases of "watchful waiting" where individuals are seen then simply moved to another waiting list, one that is not target driven. Furthermore it is apparent that methods of best practice identified a decade ago and in practice until recently are being abandoned and diluted methods are being used because they are faster and help meet targets. This Target driven system does not deliver the quality of diagnosis, nor is it followed up with adequate services. There is not a cohesive link between departments, each to a large extend, are self-focused, with a silo mentality. Supported employment is not always available and supported housing is judged on DDA criteria which does not include Autism.
Conclusion:
In conclusion PAL with the 1000 families it represents draw attention to the urgent need for joined up government to deal with the rapidly increasing number of individuals with ASD, mindful that children diagnosed with ASD grow into Adults with ASD.
A cohesive Strategy will not only stop wasteful duplication of some services, but through appropriate interventions and support greatly reduce future costs on society as individuals and families are empowered to support themselves and boost the NI economy.
Autism Initiatives NI
Autism Initiatives Northern Ireland is the largest voluntary sector provider of direct services to people with autism in Northern Ireland. The organisation employs over 200 staff and works directly with over 200 families. It is part of a UK based organisation which has its headquarters in Liverpool and has a sister organisation in the Republic of Ireland called ASD Initiatives.
Autism Initiatives Services in Northern Ireland
Supported Housing
We operate a number of schemes usually in partnership with a housing association with funding for care and support from NIHE Supporting People and/or the Health and Social Care Trust. There are 10 services providing places for 47 people and employing 123 staff located in Lisburn, Belfast, Bangor, Armagh, Newcastle and Dunmurry.
Residential
Autism Initiatives run 3 small residential facilities staffed by 48 people and providing services for a total of 24 service users, many of whom have complex physical disabilities and are frail and vulnerable. These services are based in Belfast and Newcastle including Mary Murray House, which won a People's Vote through the Big Lottery Fund to install a sensory garden.
Day Care
Autism Initiatives provides day care opportunities in its own right (and in partnership with a social enterprise business called Autism Work Ventures).
- Beechill, Belfast offers a very specialist day care experience for 3 people with complex disabilities and autism.
- Bryansford Road, Newcastle, Co.Down provides a structured day activity programme for 40 people.
- Hospital Road, Armagh offers a day care programme for 3 service users.
- Chocolate Memories, Moneyreagh is a social enterprise business making and distributing chocolate -9 service users are involved.
- Garden Centre, Newcastle -8 service users are involved with this project
- Virtual Art Gallery -3 service users who are also artists are deriving some income from selling their art work online.
There are 11 staff employed in day services. Services are offered to 68 service users (some of whom already attend some of our other services).
Community Service
We offer a wide range of community services. Outreach in Belfast for adults and children provide social opportunities for people with autism and respite for their carers. A new community house in Carryduff will be a base for these activities. We also have a 'One Stop Shop' in L'Derry and run a number of Floating Support Schemes to help service users remain in their own homes or prepare for independent living. Over 100 service users take part in activities organized through these services with about 25 staff providing support. A counselling service is offered to staff, service users and their families by volunteer counsellors who have been trained through the University of Ulster and accredited by the British Association.
In total Autism Initiatives NI provides services to well over 200 people with autism and their families. We employ about 250 people and have specialized in supporting challenging individuals who have been resettled from long-stay hospital or are perceived to be challenging, most times this is due to a lack of understanding and ability by other agencies to facilitate the person's Autism. We continue to seek new and innovative ways of providing practical support services to people with autism who are in need.
The Autism Bill
Autism Initiatives Northern Ireland have been strong supporters of the Autism Bill during the long period of its development. We believe the large numbers of people with autism and the relatively sudden increase in the identification of children and adults with the condition are strong arguments for a legislative and strategic approach. As a direct service organisation, in regular contact with families that we can help and many that we cannot, we would prefer to see the bulk of resources directed to people with autism and their families. We believe the removal of the proposal to have an advocate for people with autism is a sensible economy.
1. Amendment to the Disability Discrimination Act
The Disability Discrimination Act made it unlawful to discriminate against a disabled person. The definition of disability is important, the Act says: 'a person has a disability for the purposes of this Act if he has a physical or mental impairment which has a substantial and long-term adverse effect on his ability to carry out normal day-to-day activities.'
This definition is further clarified in schedule 1 of the Act with the listing of a number of characteristics that help define what a disability is. There is evidence from employment tribunals that discrimination cases have often focused on whether a claimant was a disabled person or not.
The proposed amendment to insert the words 'social (including communication)' into the definition in Section 1 of the Act seem sensible to us. Similarly the proposed addition of 'taking part in normal social interaction; or forming social relationships' also seem to be helpful clarifications.
Autism is a spectrum condition and the range of the condition is very wide. Many people with Autism already demonstrate that they have difficulties with carrying out normal day to day activities. These amendments make this more explicit and will also clarify that other people with Autism have a condition that can be disabling. Not all people who have Autism are necessarily disabled according to the definition of the DDA because their Autism may not prevent them from carrying out normal day to day activities. There are, however, people with Autism where the effect of their condition is hidden and they can have enormous difficulties with daily living but do not appear to be disabled.
2. Autism Strategy
We support the proposed Autism Bill as it sets out the need for an Autism Strategy across the full range of Government departments and activities. Health and Social Care will be the service providers of last resort for people with Autism unless other departments and agencies are involved fully in an Autism strategy.
Autism Initiatives Northern Ireland are enthusiastic participants in the implementation of the Regional ASD Strategy set out by the Minister for Health, Social Services and Public Safety. We would like to pay tribute to the work of Dr Stephen Bergin and Lord Maginnis for the work they have done to date and look forward to working with them further in the future. The Regional Strategy allows for the involvement of other departments and agencies and this has included Education professionals, the Department of Employment and Learning, DSD and others. A more formal requirement for involvement and co-operation would be valuable –especially at a time of acute financial concern. The temptation will surely be for departments to restrict their activities to their statutory responsibilities rather than to co-operate across departmental boundaries.
If this full co-operation does not happen the risk remains that people with Autism may find that they do not get the support they need. These could be people who might thrive in ordinary community life. But as a result of not getting the right support they may find themselves lacking support and therefore develop mental health problems or get in trouble with the law and need more extensive intervention in the future. There is a specific need for the Department of Health, Social Services and Public Safety and the Department of Education to explore how they can work more closely together and perhaps join up their services more completely.
2. (3) The collation of data on the prevalence of Autism is essential to enable the proper planning of services to take place. As noted earlier Autism is a spectrum condition. The identification of numbers of people with the condition is not enough. The production of statistics should also include some means of identifying future need. For example it may be surmised that a child with Autism who is being educated in a grammar school may have less need for supported living services in the future than a child educated in a special school. This is an inexact science of course. It does seem clear to us that while much attention is often focused on children with Autism the fact remains that kids with Autism grow up!
3. Content of the Autism Strategy
We agree with all the elements of this section of the Bill. The recognition that people with Autism have needs throughout their lives is particularly important. In paragraph 4 and paragraph 5 there are proposals for an awareness campaign for the public and awareness training for civil servants. As we said earlier we would prefer to see resources directed to services for people with Autism. As a result we would prefer to see awareness raising and training carried out as part of general disability awareness campaigns. Equality Schemes, Audit of Inequalities and public campaigns by the Equality Commission may meet the same objectives set out in these clauses without diverting resources from the Department of Health, Social Services and Public Safety.
Aspergers Network
We as an ASD Charity have watched the passage of the Autism Bill over this past year; and have had growing concerns over its content, and construction as it has passed along; and it must be mentioned at this stage, we cannot give it our backing or support One of the biggest deficits in this past year has been the severe lack any of detail about the Services for any Parent/Carer, or any individual having been mentioned; and in particular the lack of clarity as to whether this Bill will produce any intervention. This Bill has caused huge divisions; and not only with Autism families; but also within the disability world. Any individual or Charity who speaks against the Bill leaves themselves open to verbal attack.
We acknowledge how genuinely hard our politicians have strived to get things improved for those with Autism, and their families.
Our fears are based in numerous areas.
Given the fact that over twenty Charities in Northern Ireland do deliver services to different degrees for Autism, it speaks volumes that essentially one main Charity has been the driver behind its passage.
We hope to give brevity to this submission, and instead of providing all documents in a range we will only attach the required documents to help you in your considerations.
The Disability Discrimination (Northern Ireland) Order 2005 was correctly and rightly given out to
(A) Public Consultation (700 Consulted0
(B) Financial Effects of the Order
(C) Human Rights Compatible
(D) Impact Assessed
(E) Section 75 Assessed
(F) Equality Commission Involved as to Review and Advice. Major deficits are apparent.
The Autism Bill does not appear to have any of these same safe guards in place.
On the 7th December Mr D Bradley MLA said "More recently, in March and April 2010, consultation on the proposed legislation was conducted across statutory and voluntary agencies, resulting in a 70% to 80% positive rating for legislation. We held follow-up meetings with the Equality Commission, the Children's Commissioner and Disability Action. Autism touches the lives of a staggering 68,000-plus people".
There was no public Consultation whatsoever, and considering this Bill will affect quote
"a possible 68,000 people" why no public Consultation; and why was there such a ineffectual and unprofessional Consultation carried out for such an important subject.
Also a full Public Consultation should be over a twelve week period as required by the Governments own Code of Practice i.e., Sedley Requirement; Equality Commission Guidelines; when and if it comes.
As far as the Consultation that was carried out was concerned; eleven Autism related Charities were sent the Consultation and only three responded.
Again from the three leading Equality and Human Rights groups in Northern Ireland i.e., Human Rights Commission Equality Commission, and Pils; all three declined to respond; which gives us great cause for concern.
This is a Consultation which claimed a 70% return; but if fact four Autism Branches were added, plus two Anon; which were not on the list of Consultees; and this skewed the figures. How did six Responses appear when they were not consulted? The correct figures should have stated a 50% return.
The fact that Autism NI, PAL, and four Branches of Autism NI were all included in the responses list this gave Autism NI Six Votes which allowed them a block vote of 25% of all Respondents to the Consultation.
The resulting figures of 70 to 80% positive rating; which Mr Bradley eluded to; does not stand up; taking into account the way the figures were presented, and given that 25% came from on one source Autism NI. If the figures were downsized by this 25%; then the positive rating for the Legislation in the consultation would only be 45 to 55%.
Another question; why did the other fifteen branches not take part in the Consultation?
Another important factor is that the true response figure for Autism Related Charities was 20%. The vast majority 80% did not respond. At least 45% of Autism related Charities did not even receive a Consultation Document.
Whilst we have no difficulty with Autism NI; we do have a major difficulty with allowing this Consultation to influence anyone without the knowledge that the figures are not in any way a credible reflection of the Autism community. Nor are the percentages in any way correct as presented.
No Financial effects are available, and considering the Bill requires public servants, who deal with the public are to be trained; at what cost. Will these costs be removed from the recent increase in Trust services for families? Or would there be a decrease in the new Autism related jobs within Trusts?
There has been no Equality Impact Assessment been carried out.
Also Regulations and orders to be made under the act would they be made without the views and needs sought from the 68,000 individuals affected by any future changes.
Also the All Party Assembly Group Stated that under the Consultation that they required a minimisation of duplication of resource allocation; yet we have a RADSN Strategy ongoing this past two years then why is this Bill appearing to go down the same pathway of duplicating, and recollecting the same information that has been already scoped. The APAGA also stated about training yet we have spent many millions on Middletown's training, along side Dept of Education, and Voluntaries, which runs into hundreds. The SIGN Guidelines document was imbedded into RADSN; many months ago; and yet the APAGA document is still talking about training functions across all sectors
It is also obvious that some Trusts have already spotted the fact that this Legislation is supportive only of one Disability; and the fact that their scarce resources and time may be diverted to defending Legal challenges. This would be under Section 75, showing an inequality which Trusts would have to try and defend, and they would all be liable.
I think the Equality Commissions Remit must be looked at in this affair. (www.equalityni.org)
Their duties are wide and varied, and make recommendations to government on ways in which they can be improved, but in the case of the Autism Bill they have not made those recommendations. Also these duties on public authorities include the production and review of Equality Schemes, conducting equality impact assessments and including consultation as an integral part of the policy-making process. One of their priorities for Legislative reform in Northern Ireland is to keep the DDA 1995 under review; and also includes Section 75.
To change the Main Elements of the DDA's general definition, by describing and detailing Physical or Mental impairment may weaken the legal status of the DDA completely, as this has generally been its strength. This is the advice from the Equality Commission. To quantify and qualify the condition we could find that some individuals may fall outside these impairments. Taking part in Social activities may exclude some, or their social exclusion may not fit in other cases.
To be social, or retain friendship; or even be a member of a social group may even work against our individuals. To redefine the DDA would actually eliminate many on the Spectrum. The many complexities of this condition cannot be prescriptive, or it will exclude some. The Law was set to include all with the Diagnosis of Autism, Aspergers Syndrome and not exclude individuals; which could be the case in the future. No amendment over this last fifteen years has redefined any condition, for this reason. (Disability Discrimination Act 1995)
The knock on effect would also be to DLA applications; of which we have successfully won every case at Tribunal on Aspergers Syndrome. The DLA cases can and are fought on the effects of the condition its self, and the Law as it stands at the moment. If we change it we think it will be to the detriment of the individual's rights that now exist. The question number 8 in the consultation document on DLA in the Consultation was misleading: as it are the impairments on the individual and their Care Needs those gains a DLA award; and not their Disability.
As far as the Autism strategy is concerned there has been RADSN for coming up on two years now; and this includes the Reference Group. Autism NI sits on this group, as do many of her members; and also many PAL members including their Vice Chairman.
The thing that is very important about the Reference Group is that in its make up there are thirty Parent/Careers and individuals with Autism, plus service users; and they are working on the full range of services. These cover, to name a few, Health Visiting at two years old to Children and Adult Pathways, and also Transitions, assessment criteria, training, and interventions. Also they are involved in service design and delivery.
There is also the factor that RADSN works under Personal and Public Involvement; whereby the Department's commitment to strengthening the voice of those who use the services and ensuring the public has a stronger voice in priority setting and decisions is a new Statutory Duty. (www.dhsspsni.gov.uk/hsc_sqsd_29-07.pdf)
We don't think removing those Legal rights would be the thing to do, as these individuals are competent and have a professional attitude towards improving the Autism services in Northern Ireland. To remove their voices in Autism matters would be a retrograde step.
The lack of any particular clause regarding co-morbid conditions; or what we would describe as dual diagnosis is concerned; is so low on the radar that these multiplicities of conditions are nowhere to be seen on the Bill. So by changing a DDA and Writing an already written Strategy, surely the question is how where and when do we address these other conditions. Nearly every one of our individuals with ASD, suffer from some add on condition. It can be, ADHD, ADD, ODD, OCD, Epilepsy, Downs Syndrome Diabetes, Sensory Difficulties, Anxiety etc., (www.en.wikipedia.org/wiki/conditions_comorbid_to_autism_spectrum_disorders)
We cannot attempt to address Autism services in isolation; as they come under the bigger umbrella of Disability. An Autism Commissioner would not be the answer; but consideration should be given to establishing a Disability Commissioner; who no doubt could cover the Autistic Spectrum, and the complexities of all their add on conditions. Plus the Commissioner could work with the Equality Commission to amend the required laws. What we don't need is to promulgate a Hierarchy of Disabilities when Autism is separate to all other Disabilities. In the very near future we will face major cuts in Budgets in the welfare budgets and we will require as many friends as possible. (archive.niassembly.gov.uk/10/research/2008/5208.pdf) We feel that the Equality Commission must be heard at the HSSPS Committee, as Mr. Wells suggested in December 2010.
A quote from Mr. Jim Wells on the 7Th December 2010
"As with any Bill, the Committee will take evidence from key stakeholders who are involved in providing services to children and adults with autism and from organisations that may be affected by the Bill. The Committee recognises that complex issues are in play and that there are different opinions on the various aspects of the Bill. We will listen carefully to all views and come to our decisions on the basis of the evidence that is put before us".
We would ask the Committee for an Oral Hearing, as we are as passionate as the Committee to get these issues correct; and to ensure we definitely do not get it wrong.
PEAT
Parents' Education as Autism Therapists (PEAT)
www.peatni.org
Chairperson: Dr Tony Byrne tony@peatni.org
Comments on the Draft Autism Bill for Northern Ireland
In principle, PEAT agrees there is a need for legislation to protect the rights and interests of persons diagnosed with Autistic Spectrum Disorders (ASD) and their families or carers. PEAT is aware that the HSC already has an ASD strategy which came following the review of HSC Autism provision chaired by Lord Ken Maginnis (Maginnis, K.(2008) Independent Review of Autism Services). However, PEAT was not consulted concerning this review and again we raised our concerns in relation to the "AUTISM SPECTRUM DISORDER (ASD), STRATEGIC ACTION PLAN, 2008/09 – 2010/11" (see Annex I). Indeed PEAT, in collaboration with Queen's University Belfast and the University of Ulster, published a research report "Meeting the needs of families living with children diagnosed with ASD" in 2007 which focused on families in Northern Ireland (Annex II). This report, although made readily available was ignored by the Maginnis review.
The priority for ASD in Northern Ireland should be effective treatment and intervention. The Health Committee should consider a truly independent review of ASD services which would be open, transparent and take account of international best practice. As a starting point, the Health Committee should look at recent happenings in the USA and Canada in relation to ASD provision. For example, Ontario will be expanding services for children with autism-spectrum disorders starting next spring. The province will spend $25 million a year to provide Applied Behaviour Analysis services and supports in community agencies and centres, schools and homes (Canadian Press, 14, 12, 2010). In the USA, to date 31 States have passed autism insurance legislation which will require health insurance policies to cover the diagnosis and treatment of autism spectrum disorders, and require health insurance companies to pay for evidence-based early intervention, widely recognised as Applied Behaviour Analysis.
Applied Behaviour Analysis intervention is not a statutory right for children with ASD in Northern Ireland and families must pay privately for such intervention, which is therefore not regulated. Given the investment and legislation in the USA and Canada, obviously there is a strong economic argument for effective intervention based on ABA. Indeed there have been several cost-based analyses reported on the use of early intervention based on ABA and all conclude that there would be significant cost savings in the long term. For example, Motiwala et al (2006) reported that the use of early intensive ABA would reduce the total costs of care for autistic individuals and increase the gains in dependency-free life (Annex III). Chasson et al. (2007) reported estimated cost savings in the region of $2.09 billion for the State of Texas alone if early intensive ABA was funded for the existing children with ASD, as opposed to existing (eclectic) special education provision (Annex IV). There are a number of reports concerning the cost of provision over the lifetime of a child diagnosed. For example, Knapp et al. (2007) reported on the cost of ASD in the UK. The aggregate national costs of supporting children with ASD were estimated to be £2.7 billion each year. Most of this cost is accounted for by services used. For adults, the aggregate costs for adults amount to £25 billion each year. Of this total, 59% is accounted for by services, 36% by lost employment for the individual with ASD, and the remainder by family expenses (Annex V).
If the proposed Autism Bill will ensure that effective treatment and intervention for children and adults with ASD will be delivered in Northern Ireland, then it will have the full support of PEAT.
Yours sincerely
Dr Tony Byrne 6 January 2011
On behalf of the PEAT Charity
Department for Regional Development
South Eastern Education and Library Board (SEELB)
1. SEELB recognises the need for continued support services for people with autism in their transition from education to adult life.
2. SEELB acknowledges and supports the work that DE, DHSSPS and ELBs are already doing to develop co-ordinated Autism Strategies for children and adults.
3. The special educational needs and provision requirements of children and young people with autism are already provided for through existing Special Educational Needs (SEN) and Disability legislation.
4. Should the Autism Bill (N.I.) 2010 relate to children and young people it would give rise to complexities and possible conflicts with existing SEN and Disability legislation.
5. Difficulties would be created in relation to existing Disability Discrimination legislation if children with Autism were to be given special and preferential legislative treatment relative to children with any of a wide range of other conditions covered by SEN and Disability legislation, e.g. Down Syndrome; Dyslexia; Attention Deficit Hyperactivity Disorder (ADHD).
6. Unnecessarily complex accountability structures would be created for DHSSPS, DE and ELBs, diverting resources away from frontline services for children and adults with autism.
7. After careful consideration of these issues in England it was decided that, to avoid unnecessary complexities in legislation and to best serve the needs of both children and adults with autism, the Autism Act (2009) would relate to adult services only.
8. SEELB would recommend a similar arrangement in relation to the Autism Bill (N.I.) 2010.
9. To this end, SEELB recommends that Clauses 3 (1), 3(2) and 3(3) of the Bill be amended to replace the word "persons" with the word "adults".
10. The definition of Autism in Clause 4 (1) is likely soon to become outdated with the planned introduction of amendments to international diagnostic classification manuals. For this reason, in the Autism Act 2009 (in England) and the Autism (Scotland) Bill 2010, a definition has not been included in the primary legislation, but is to be included in the (updateable) Autism Strategy. SEELB is of the view that a similar arrangement should apply for the Autism Bill (N.I.) 2010 and therefore recommends that Clause 4 (1) be amended to remove a definition of autism from the Bill.
Belfast Education and Library Board
1 The Committee for Health, Social Services and Public Safety has asked for comments on the amendments to the Autism Bill. The Belfast Education and Library Board welcomes the opportunity to be part of the consultation and would make the following points in regard to the proposed amendments to the Bill.
2 DE and DHSSPS and the Education and Library Boards are already involved in the development of co-ordinated Autism Strategies and they are aware of the need for interdepartmental and multi-agency co-operation in order to achieve a co-ordinated Autism Strategy. The Belfast Education and Library Board fully supports this and recognises the potential value of these activities, but remains concerned that ASD specific legislation in relation to children could inadvertently discriminate against all other children with special educational needs.
3 Similar legislation was advocated in England last year and the outcome was the Autism Act (2009). Initially it was proposed that the English legislation should contain clauses relating to services for children and young people, but ultimately the Autism Act (2009) referred to adult services only. The Autism Bill (NI) relates to persons with autism throughout their lives. This will introduce considerable complexity as the Bill will have to be compatible with an already complex body of Special Educational Needs and Disability legislation relating to children. If the Assembly wishes to pursue the Autism Bill (NI) 2010 they may wish to consider restricting the Bill to adult services.
4 The implementation of autism legislation here, if it impinges on legislation that relates to the education of children, would create problems with regard to equity. Existing Special Educational Needs and Disability legislation protects the rights of children experiencing a broad range of Special Educational Needs and Disabilities, for example, Severe and Moderate Learning Difficulties, Down Syndrome, Attention Deficit with Hyperactivity Disorder, Specific Learning Difficulties/Dyslexia, Medical/Physical difficulties, Visual and Hearing Impairments. This legislation also relates to children whose difficulties arise from Autistic Spectrum Disorders. The Equality Commission (eg in their Code of Practice for Schools) clearly regard Autism as already coming within the terms of the Disability Discrimination Act. It is difficult to justify special legislative treatment of the needs of children experiencing Autistic Spectrum Disorders (ASD) in preference to special legislative treatment of the needs of the many other children with Special Educational Needs and Disabilities.
5 ASD encompasses a very broad spectrum of impairments which vary greatly in severity. Within the education sector for some children ASD may present a very mild obstacle to learning while others may experience very severe obstacles. Schools and Education and Library Boards (ELBs) need to respond in a graduated manner in response to these varying needs. Autism specific legislation could create or reinforce the notion that if a child has an ASD diagnosis then the child must have one particular type or level of assessment and support.
6 It is proposed in the amendments to the Bill that the DHSSPS will have overall responsibility for the development of the Autism Strategy but DE (and hence the ELBs) must implement that part of the strategy which falls within its area of responsibility. DHSSPS will be required to monitor the implementation of the strategy by DE/ELBs and report to the Assembly on the progress made by DE/ELBs. This is a complex accountability structure and reporting mechanism which appears to make DE/ELBs accountable to the DHSSPS. If the Bill was to be restricted to adult services this would remove these potential difficulties
7 Autism is not defined in the Autism Act 2009 in England. Rather the definition is reserved for subsequent strategy documents which can be amended over time as required as the conditions associated with Autism become better understood. This was done because the terminology used around Autism does change over time. For example in the next version of the internationally recognised diagnostic criteria (DSM V, as opposed to the current DSM IV) it is probable that the term Asperger's syndrome will not be used and it is already becoming commonplace for the term "Autistic Spectrum Conditions" to be used in preference to Autistic Spectrum Disorder (ASD).
Southern Health & Social Care Trust
Southern Education and Library Board and Western Education and Library Board
This represents a response on behalf of both the Southern Education and Library Board (SELB) and the Western Education and Library Board (WELB). Both Boards welcome the opportunity to comment on the Autism Bill as follows:-
Co-ordinated Strategy:
The need for a co-ordinated Autism Strategy between Health and Education Departments is widely accepted. At this stage, considerable progress has been made in respect of inter-departmental co-operation and work to develop a co-ordinated Autism Strategy. The planning in relation to this work has already begun by both Health and Education. Further benefits are envisaged in the future for children and young people who have Autism, in the absence of an Autism Bill, through the implementation of a co-ordinated Autism Strategy.
The view of SELB and WELB is that an Autism Bill is unnecessary and unhelpful. There is concern that the Bill may also be potentially discriminatory for the children and young people concerned. In this regard, it is important to consider the potential pitfalls which may occur as a consequence of the creation of Autism specific legislation.
There are also real concerns that the children and young people who have other conditions may also require specific legislation; the equality issues which could arise in this area require judicious consideration of Special Educational Needs in general as well as in relation to Autism in particular.
Autism - Diagnostic Continuum:
Autism is a medical diagnosis and as such it is not directly related to Special Educational Need. However, many children on the Autistic Spectrum may have a Special Educational Need. This may arise from a particularly severe presentation of Autism or may arise from other conditions which co-occur with it.
Autism is a spectrum disorder and is more commonly referred to as Autistic Spectrum Disorder (ASD). There is wide diversity in presentation between individuals who share the diagnostic label and also within the same individual over time and context. Many children with a diagnosis of ASD do not have identified Special Educational Needs. Indeed, the continuum of need in relation to Autism should also be reflected in the continuum of services and provision which may be required to support children and young people.
There is a danger that the proposed Autism Bill will create an impression that children or young people by virtue of a diagnosis label are disabled. This would likely reinforce a perception that there is something inherently 'wrong' with the child or young person or that they are incompetent. This could lead not only to a loss of opportunity for each individual but to discriminatory behavior, prejudice and negative intervention responses in schools or in the workplace. Indeed, there is growing acceptance of the use of the term Autism Spectrum Conditions to avoid such a perception.
Donna Williams (1994a) author of Nobody Nowhere (1992) and Somebody Somewhere (1994b) writes:
"When people without autism assume that people with autism are merely 'slow' or 'broken' versions of themselves, they may not only insult, but additionally confuse and frustrate the person with autism with behavior that naturally stems from these arrogant and ignorant assumptions." (p. 197)
The label 'disability' is not neutral. It has the potential to have significant social, emotional, educational and employment consequences for individuals with Autism.
Existing Education Legislation:
The educational legislation governing the assessment and identification of Special Educational Need does not promote a 'medical model' approach as this would be considered inconsistent with the philosophy of individualisation of assessment, identification and intervention. The educational approach is framed within a contextual model. Special difficulties and needs are assessed in the context of the environment and circumstances of the child or young person.
One of the functions of existing ASD services is to support parents and schools in making appropriate adjustments to the environment to accommodate the different processing styles of children and young people with ASD. In this respect, the child or young person is not perceived as 'the problem'. The focus shifts to that of the environment and the extent to which it accommodates the identified needs of each individual. Many factors outside of a diagnosis of Autism determine the likelihood of a disability.
Impact on Children and Young People:
It is the experience of the ASD Services in SELB and WELB that many children and young people with a diagnosis of ASD do not perceive themselves as having a disability. They consider that there are positive strengths to their condition. Indeed, they are encouraged in this regard by their parents, school and the ASD Service. The idea that they may now be required to refer to their 'disability' rather than a 'condition' would likely cause considerable anxiety and distress in their struggle against the associations which such a label could bring. It could also block the essential focus of the ASD Services which has been to promote inclusion through adjustments and accommodations. Simply, the label of 'disability' does not reflect the real life experiences of many children and young people with Autism.
The needs of children and young people with ASD require a graduated response not a categorical one. These children and young people do not require special legislative treatment.
Conclusion:
As statutory and voluntary bodies work to support the continuing development of children and young people with Autism there is increased confidence and competence that this can be delivered within existing supports and provisions without Autism specific legislation.
Equality Commission for Northern Ireland
Introduction
1. The Equality Commission for Northern Ireland ('the Equality Commission') is an independent public body established under the Northern Ireland Act 1998. The Commission is responsible for implementing the legislation on fair employment, sex discrimination and equal pay, race relations, sexual orientation, disability and age. The Commission's remit also includes overseeing the statutory duties on public authorities to promote equality of opportunity and good relations under Section 75 of the Northern Ireland Act 1998 and the disability duties under the Disability Discrimination Act 1995.
2. In addition, the Equality Commission, along with the Northern Ireland Human Rights Commission, has been designated under the U.N. Convention on the Rights of Persons with Disabilities ('UNCRPD') as the independent mechanism tasked with promoting, protecting and monitoring implementation of the UNCRPD in Northern Ireland.
3. The Equality Commission welcomes the opportunity to submit evidence to the Health, Social Services & Public Safety Committee ('the Committee') in relation to the Autism Bill. In responding to the Committee's invitation to submit evidence, the Equality Commission draws on the experience it has gained in advising complainants (including complainants with autism) in relation to disability discrimination under the Disability Discrimination Act 1995 (DDA 1995) and Special Educational Needs and Disability (NI) Order 2005 (SENDO 2005) .
4. We note that the Bill proposes to amend the DDA 1995 with the aim of resolving any ambiguity as to whether the term 'disability' applies to autistic spectrum conditions, and to require the preparation and implementation of an autism strategy. Our comments in relation to both of these proposals are set out below.
Amendments to the Disability Discrimination Act 1995.
5. Clause 1 of the Autism Bill proposes amendments to the DDA 1995 in relation to the definition of disability. In particular, whereas the current definition of 'disability' makes reference to having 'a physical or mental impairment', the Bill proposes to amend the definition to include reference to 'social' impairments, which are to be interpreted as including communication difficulties.
6. The current definition of disability within the DDA 1995 defines a disabled person as a person with a physical or mental impairment which has a substantial and long term adverse affect on his/her ability to carry out normal day-to-day activities. The DDA 1995 also states that an impairment is to be taken to affect the ability of a person to carry out normal day-to-day activities only if it affects that person in respect of one or more of the following:-
- mobility;
- manual dexterity;
- physical co-ordination;
- incontinence;
- ability to lift, carry or otherwise move every day objects;
- speech, hearing or eyesight;
- memory or ability to concentrate, learn or understand; or
- perception of the risk of physical danger.
7. The above list is referred to as a list of 'capacities'.
8. Clause 1 of the Autism Bill proposes to extend the list of capacities within the definition of 'normal day-to-day activities' in Schedule 1 so that a condition which has a substantial and long term adverse affect on someone's ability to take part in normal social interaction or to form social relationships can constitute a 'disability'.
9. These amendments have been proposed to the definition of disability in order to clarify that the DDA 1995 adequately embraces autistic spectrum conditions.
10. The Equality Commission recognises that people with some mental health conditions may be excluded from the definition of disability within the DDA 1995. In 2003, the Commission made a series of recommendations for change to the DDA 1995 in 'Enabled?'[1] which included recommendations in relation to the definition of disability.
11. In Enabled?, the Equality Commission recommended that the list of normal day-to-day activities should be revised to include 'the ability to communicate and interact with others' and to ensure that self-harming behaviour is covered. In Enabled?, the Commission cited examples of people with mental health conditions (not autism) who had been deemed by courts and tribunals not to fall within the definition of disability. These conditions included Post Traumatic Stress Disorder, depression and Bulimia Nervosa.
12. From its experience of dealing with complaints of disability discrimination both under the DDA 1995 and SENDO 2005, the Commission is not aware that the definition of disability within the DDA 1995 has caused particular difficulties for people with autism accessing their rights under the legislation. The Commission has supported a number of complainants (both adults and children) with autism, and it has not been the Commission's experience that Respondents in those cases have alleged that the complainants have failed to meet the definition of disability within the DDA 1995.
13. In addition, it will be noted that the Office of the First Minister and Deputy First Minister (OFMdFM) has issued Guidance on matters to be taken into account in determining questions relating to the definition of disability,[2] which concerns the definition of disability within the DDA 1995, and which is also used in Part III of the SENDO 2005.
14. The DDA 1995 requires that courts and tribunals must take into account any aspect of this Guidance which appears to be relevant when deciding whether or not a person is disabled under the DDA 1995.
15. As made clear in the examples cited in the OFMdFM Guidance, autism can affect one or more capacities listed in the definition; including speech, hearing or eyesight; memory or ability to concentrate, learn or understand; or perception of the risk of physical danger.
16. In particular, the OFMdFM Guidance includes under the section which gives examples on the capacity 'memory or ability to concentrate, learn or understand', an example of a man with Asperger's syndrome, a form of autism, who has difficulty in communicating with people.
17. The Guidance makes it clear that 'the ability to learn or understand also covers the perception of what is meant by certain types of verbal communication such as the use of humour or sarcasm as well as non-verbal communication such as body language and facial expressions'.
18. The OFMdFM Guidance also includes an example of a six year old child who has been diagnosed as having autism, who has difficulty communicating through speech and in recognising when someone is happy or sad. It confirms that this amounts to a substantial adverse effect on his ability to carry out normal day-to-day activities, even for such a young child. It states that the capacities of mobility, speech and perception of risk are all affected.
19. It will also be noted that the Equality Commission's Code of Practice for Schools[3] on SENDO 2005 includes an example of a pupil with Asperger's syndrome and a pupil with autism.
Changes in Great Britain
20. The Committee will be aware that changes have been made in Great Britain to the definition of disability under the Equality Act 2010. In particular, the definition of disability in the Equality Act 2010 amended the definition of disability by removing the list of capacities; thereby making it easier for disabled people to fall within the definition of disability.
21. It did not, as proposed by the Autism Bill, amend the definition so as to clarify that people with autism were covered by the disability legislation.
22. The definition of disability (as amended) within the Equality Act 2010 came into force on 1 October 2010. It will be noted that the Office of Disability Issues in Great Britain undertook a consultation on the Guidance on the definition of disability under the Equality Act 2010 (as oppose to the definition of 'disability'), which finished at the end of October 2010[4].
23. The draft Guidance on the definition of disability under the Equality Act specifically states that a disability can arise from a wide range of impairments which can be 'developmental, such as autistic spectrum disorders (ASD), dyslexia and dyspraxia'. It also includes examples of a child with autism, and a man with Asperger's syndrome. It further includes, in the Appendix, an illustrative and non-exhaustive list of factors which, if they are experienced by a disabled person, it would be reasonable to regard as having a substantial adverse effect on normal day-to-day activities. These factors include 'significant difficulty taking part in normal social interactions or forming social relationships'.
The way forward
24. As highlighted above, the Equality Commission has previously recommended, in recognition of the fact that people with some mental health conditions (though not specifically autism) may be excluded from the definition of disability within in the DDA 1995, a change to the definition of disability so normal day-to-day activities should be revised to include 'the ability to communicate and interact with others'.
25. In line with changes that have occurred in Great Britain (GB) under the Equality Act 2010, rather than adding to the current list of capacities, as advocated in the Autism Bill, one alternative approach for consideration is the removal of the list of capacities in total from the definition of 'disability' within the DDA 1995.
26. It will be noted that the UK Government in its response to the consultation on the Equality Bill[5] outlined its reasons behind its proposal to remove the list of capacities. In particular, it stated that its decision was based on evidence indicating that the list served little or no purpose in helping to establish whether someone was disabled in the eyes of the law, and was an unnecessary extra barrier to disabled people taking cases in courts and tribunals.
27. It further indicated that the list of capacities had led to some confusion, and had frequently been misinterpreted as a list of day-to-day activities. The Government also indicated that there was evidence that it can be harder for people with a mental health condition to demonstrate their impairment's effect in one of these capacities; although the Government recognised that the revised statutory guidance on the definition of disability had alleviated this difficulty.
28. In deciding to repeal the list of capacities, the Government stated that removing the list of capacities also simplified the definition of disability. The Government stressed, in the event that the list of capacities was removed, that there was a need for clear guidance on the definition of disability in order to enable people to understand the law and their rights and responsibilities.
29. It is of note that the Joint Committee on Human Rights in its report on the Equality Bill also welcomed the deletion of the list of 'capacities' from the definition of disability which it stated will 'clarify the law and make it easier for claimants to demonstrate that they are 'disabled' for the purposes of the legislation'.[6]
30. In addition, as an alternative to incremental changes to the definition, in line with its previous recommendation in Enabled?, the Commission recommends a fundamental review of the definition of disability in order to reflect the social model of disability. This is particularly relevant in light of the fact that the United Nations Convention on the Rights of People with Disabilities (UNCRPD), which has been ratified by the UK Government, contains a non-exhaustive definition of disability which is based on the 'social model' of disability.
31. The Committee will note that the Joint Committee on Human Rights in its report on the Equality Bill indicated that there were 'strong arguments for adopting a definition of disability which is more in tune with the 'social model' of disability set out in the UN Convention on the Rights of Persons with Disabilities, rather than one based on medical conditions.' It was of the view that there was 'little risk of this change leading to abuse or trivialisation of the status of being disabled.' In particular, it recommended that the reference to 'long term' impairment should be omitted from the current definition of disability. This change is in line with the Equality Commission's recommendations in Enabled?. However, the Committee will also note that these recommendations of the Joint Committee on Human Rights were not taken forward in the Equality Act 2010.
Reform of the DDA 1995
32. On a more general basis, the Equality Commission is of the view that greater protection for autistic children and adults (as well as other disabled people) could be more effectively secured by a major reform of the DDA 1995 and SENDO 2005.
33. Prior to the implementation of the Equality Act 2010 in GB, the DDA 1995 was a UK-wide Act of Parliament (with some modifications in relation to its application in Northern Ireland). In general, prior to the introduction of the Equality Act 2010, Northern Ireland disability equality law largely reflected GB law. However, since the implementation of the majority of the Act's provisions relating to disability on 1 October 2010, there are now significant differences between GB and Northern Ireland disability equality law.
34. Importantly, these changes will mean that disabled people in Northern Ireland will have less protection against unlawful disability discrimination, harassment, victimisation and a failure to make reasonable adjustments than those in GB.
35. The Committee will be aware that the Equality Commission has supported a number of cases in order to clarify disability equality law including the case of Elizabeth Boyle v SCA Packaging Ltd, which sought to clarify the definition of disability within the DDA 1995.[7]
36. The changes which have occurred in GB under the Equality Act 2010 will mean that there will be increased inconsistency and differences not only as regards the legislation but also in relation to emerging case law between the two jurisdictions.
37. The Equality Commission has formally submitted to Junior Ministers in OFMdFM a series of proposals for urgent legislative reform; including reform of the DDA 1995 and SENDO 2005. A copy of the Equality Commission's detailed proposals paper submitted to the Junior Ministers is available on the Equality Commission's website.[8]
Autism Strategy
38. Clause II of the Autism Bill proposes placing a requirement on the Department of Health, Social Services and Public Safety (DHSSPS) to prepare and publish a strategy on autism within two years of the passing of the Act and following consultation with the other Northern Ireland Departments.
39. Whilst recognising the need for further action across all Northern Ireland Departments to ensure that effective services for people with autism are delivered, the Commission is not convinced that there is a clear need for the DHSSPS to be placed under a duty to prepare a strategy on autism.
40. The Committee will be aware that the Department and other designated public authorities, under Section 75 of the Northern Ireland Act 1998, are already under a duty to consider the need to promote equality of opportunity for disabled and non-disabled people when carrying out their functions. Therefore, the Department and other public authorities must consider what steps it can take to promote equality of opportunity for all disabled people, including people with autism.
41. If people with autism are experiencing barriers in terms of accessing services or in terms of their specific needs not being met, there is a duty on designated public authorities to consider steps to tackle these barriers or meet specific needs. In line with the Commission's revised Section 75 Guide, the Commission has recommended that public authorities carry out an audit of inequalities across all Section 75 grounds (including disability) and that public authorities set out in an action plan, with specific actions, time scales and performance indicators, measures that they intend to take to address key inequalities (including key inequalities affecting disabled people).
42. The Committee will be further aware that the UK Government has ratified the United Nations Convention on the Rights of People with Disabilities (UNCRPD). It is therefore important that Government Departments and all other public authorities in Northern Ireland consider what steps they need to take as regards disabled people (including people with autism) in order to ensure that the obligations placed on the UK Government under the UNCRPD are fully complied with.
43. We note that the Bill proposes that the Autism Strategy must set out steps the DHSSPS proposes to take to ensure that all Northern Ireland Civil Service staff who deal directly with the public are given autism awareness training.
44. Under the DDA 1995, public authorities in Northern Ireland are under a duty to have due regard to the need to promote positive attitudes towards disabled people and to encourage the participation of disabled people in public life ('disability duties'). In pursuance of the disability duties, public authorities must produce a disability action plan in line with the Guidance on the disability duties published by the Equality Commission.[9] The Guidance makes it clear that there is one measure which a public authority must outline in its disability action plan; namely, the steps it intends to take in order to ensure that training and guidance on the disability equality legislation and disability awareness is provided to staff and office holders. This training and guidance covers all forms of disability.
45. Finally, we support a cross- departmental action plan, with clear actions, timescales, performance indicators, that delivers tangible outcomes for disabled people, which is aimed at addressing the key recommendations set out in the OFMdFM Report of the Promoting Social Inclusion Working Group on Disability.[10]
Conclusion
46. To conclude, it is clear that urgent changes are required to the definition of disability within the DDA 1995 (as well as other parts of the disability legislation) in order to ensure that disabled people have access to the law and have effective protection against discrimination. The amendment proposed in the Bill is not sufficient.
47. There is also a need for cross-departmental action to ensure effective services for people with autism. It is also essential that all public authorities in Northern Ireland comply with their obligations as regards disabled people under Section 75 of the Northern Ireland Act 1995, the DDA 1995, as well as ensuring that the Government complies with its obligations under the UNCRPD. The amendment proposed in the Bill is not sufficient.
[1] Enabled? Recommendations for change to the Disability Discrimination Act 1995, 2003, ECNI http://www.equalityni.org/archive/word/Enabledfinalpublished260603.doc
[2] Guidance on matters to be taken into account in determining questions relating to the definition of disability, OFMdFM, 2008, www.ofmdfmni.gov.uk.
[3] Disability Discrimination Code of Practice for Schools, ECNI, 2006, http://www.equalityni.org/archive/pdf/FSchoolsCOP(SENDO).pdf
[4] Office for Disability Issues, Equality Act 2010 Guidance – Guidance on mattes to be taken into account in determining questions relating to the definition of disability. http://www.officefordisability.gov.uk/docs/wor/new/ea-guide.pdf
[5] The Equality Bill-Government Response to the Consultation, Cm7454, July 2008, http://www.official-documents.gov.uk/document/cm74/7454/7454.pdf
[6] Joint Committee on Human Rights, Legislative scrutiny: Equality Bill, November 2009, http://www.publications,parliament.uk/pa/jt200809/jtselect/jtrights/169/169.pdf
[7] SCA Packaging Ltd v Elizabeth Boyle [2009] UKHL 37
[8] The ECNI proposals paper is available at http://www.equalityni.org/sections/default.asp?secid=5&cms=The+Law_Legislative+Reform&cmsid=4_285&id=285
[9] A Guide for Public Authorities- Promoting Positive Attitudes Towards Disabled People and Encouraging the Participation of Disabled People in Public Life, ECNI, 2007 http://www.equalityni.org/archive/pdf/ECNIDisPlan.pdf
[10] Report of the Promoting Social Inclusion Working Group on Disability, www.ofmdfmni.gov.uk, December 2009
Action for Children NI
I am writing to you in response to your letter to Dawn Shaw (10th December 2010) and the NI Assembly Autism Bill. In addition to some information about Action for Children, our response below includes some general points and suggestions (in italics) regarding the Bill and its Clauses.
Action for Children works with children and young people who most need support to achieve their full potential. This includes providing services for children and young people whose families need support, who cannot live with their birth families, who are disabled and who experience severe difficulties in their lives. Through our services and campaigns, we challenge injustice, deprivation and inequality, and seek to empower children to overcome the obstacles in their lives that hold them back.
Across the UK, Action for Children is a major provider of services to disabled children and we currently run over 60 projects providing specialist services for disabled children in partnership with local authorities and other providers in GB in addition to over 9,000 disabled children accessing our other inclusive children's services.
Our specialist disability services include domiciliary care, residential short breaks, residential care and schools, Children's Centres, transition support, key working, advocacy, shared care short breaks, and inclusive play and leisure activities. A significant number of children using our services have challenging behaviour, complex health needs or life-limiting illnesses.
While we do not currently provide any specialist disability services in Northern Ireland, we are interested in developing such services as part of our portfolio of services addressing the needs of the most vulnerable and marginalised children and young people. We work in close partnership with a number of disability organisations in helping support families of disabled children including children on the Autism Spectrum.
Action for Children believes there should be a legally enforceable duty placed on statutory / local authorities to ensure that services are responsive, flexible and of a high-quality and that each service must be provided to each disabled child, young person and their family based on a true assessment of need.
Action for Children supports the primary intention of the NI Assembly Autism Bill and its key Clauses focused on enhancing provision of services and support for people on the autism spectrum through a) amending the Disability Discrimination Act 1995 in order to resolve any ambiguity as to whether the term "disability" applies to autism spectrum conditions and b) requiring the preparation and implementation of an autism strategy in Northern Ireland, led by the Department of Health, Social Services and Public Safety (DHSSPS) but with full cooperation of other government departments and sectors.
Amendment to the Disability Discrimination Act 1995
We note that Clause 1 seeks to amend the Disability Discrimination Act 1995 ("the Act"), a UK piece of legislation, through amending the definition of disability in "the Act" to include reference to 'social' impairments which are to be interpreted as including communication difficulties. We note also that Clause 1 seeks to extend the definition of "normal day-to-day activities" in Schedule 1 so that a condition which has a substantial and long-term adverse effect on someone's ability to take part in normal social interaction or to form social relationships can constitute a "disability".
Autism Strategy – Development, Implementation and Content
We note Clause 2 requires the DHSSPS ("the Department") to prepare and publish a strategy on autism within 2 years of the passing of the Act and following consultation with the other Northern Ireland Executive departments - who are placed under an obligation to implement any part of the strategy for which they are responsible. However, the strategy must be accompanied by statutory duties on local agencies such as Health and Social Care Trusts and Education bodies to deliver service improvements for people on the autism spectrum, and those with Aspergers syndrome in particular.
Action for Children believes it is essential that Northern Ireland government departments and their agencies should be required to co-operate in the preparation, implementation and review of any such strategies with the Minister reporting to the Assembly every three years.
With regard to the content of the autism strategy, we note Clause 3 sets out how the needs of people with autism spectrum conditions are to be addressed throughout their lives. We welcome this 'lifetime' and holistic focus and believe the autism strategy should pay particular attention to key 'transition' issues facing children and young people on the autism spectrum. In doing so, the strategy should consider the challenges many older young people may face when making the move toward adulthood and 'independence' and the need for ongoing support from adult services.
We note too that the autism strategy must identify what steps the Department propose to take to promote an autism awareness campaign and also what training measures are to be taken with the Northern Ireland Civil Service staff who interface with the public on such issues.
I hope you find this submission of assistance to the Committee's consideration of the Bill and need for any amendments to it.
North Eastern Education and Library Board
1. General Comments
1.1 While a similar proposal was advocated in England last year the resultant Autism Act (2009) related only to an autism strategy for adults in England. The original Bill contained clauses that would strengthen services for children and young people but the Government agreed to meet these clauses outside the provisions of the Bill.
1.2 The implementation of autism legislation in Northern Ireland, which includes legislation that relates to the education of children, would create problems with regard to equity.
1.3 ASD encompasses a very broad spectrum of impairments which vary greatly in severity. ASD may present a very mild obstacle to learning for some children ranging through to a very severe obstacle for others. Schools and Boards need to respond in a graduated manner in response to these varying needs.
1.4 DE and DHSSPS are already involved in the development of co-ordinated Autism Strategies and are well aware of the need for interdepartmental co-operation. While the NEELB recognises the potential value of these activities it does not consider that new legislation specific to ASD is needed in order to achieve a co-ordinated Autism Strategy.
2. Amendment to the Disability Discrimination Act 1995
2.1 Similar legislation was advocated in England last year and the outcome was the Autism Act (2009). Initially it was proposed that the English legislation should contain clauses relating to services for children and young people, but ultimately the Autism Act (2009) referred to adult services only. The Autism Bill (NI) relates to persons with autism throughout their lives. This will introduce considerable complexity as the bill will have to be compatible with an already considerable body of Special Educational Needs and disability legislation relating to children.
2.2 The implementation of autism legislation here, if it impinges on legislation that relates to the education of children, would create problems with regard to equity. Existing Special Educational Needs (SEN) and disability legislation protects the rights of children experiencing a broad range of Special Educational Needs and disabilities, for example, Severe and Moderate Learning Difficulties, Down syndrome, Attention Deficit with Hyperactivity Disorder (ADHD), Specific Learning Difficulties/Dyslexia, Medical/Physical difficulties, Visual and Hearing Impairments. This legislation also relates to children whose difficulties arise from Autistic Spectrum Disorders (ASD). The Equality Commission (e.g. in their Code of Practice for Schools) clearly regard Autism as already coming within the terms of the Disability Discrimination Act. In the Board's view it is inappropriate to make special legislative provision for the needs of the broad spectrum of children experiencing ASD in preference to the needs of the many other named groups of children with SENs/disabilities.
2.3 ASD encompasses a very broad spectrum of impairments which vary greatly in severity. ASD may present a very mild obstacle to learning for some children ranging through to a very severe obstacle for others. Schools and Education and Library Boards (ELBs) need to respond in a graduated manner in response to these varying needs. Autism specific legislation may create or reinforce the notion that if a child has an ASD diagnosis then the child must have one particular type or level of assessment and support – and because they have the ASD label they should have preferential treatment over other children with SENs/Disabilities.
2.4 The label 'disability' is not neutral. It will likely have significant social, emotional, educational and employment consequences for individuals with ASD.
2.5 The educational legislation governing the assessment and identification of Special Educational Needs does not promote a 'medical model' approach as this would be considered inconsistent with the philosophy of individualisation of assessment, identification and intervention. The educational approach is framed within a contextual model. Special difficulties and needs are assessed in the context of the environment and circumstances of the child or young person. One of the functions of the ASD services is to support parents and schools in making appropriate adjustments to the environment to accommodate the different learning styles of children and young people with ASD. In this respect, the child or young person is not perceived as 'the problem'. The focus shifts to that of the environment and the extent to which it accommodates the identified needs of each individual. Many factors, outside of a diagnosis of autism, determine the likelihood of a disability.
3. Interpretation
3.1 Autism is not defined in the Autism Act 2009 in England. Rather the definition is reserved for subsequent strategy documents which can be amended over time as required as the conditions associated with Autism become better understood. This was done because the terminology used around Autism does change over time. For example in the next version of the internationally recognised diagnostic criteria (DSM V, as opposed to the current DSM IV) it is probable that the term Asperger's Syndrome will not be used and it is already becoming commonplace for the term "Autistic Spectrum Conditions" to be used in preference to Autistic Spectrum Disorder (ASD).
Carers NI
Introduction
We are pleased to have an opportunity to assist the Committee in considering the potential for the proposed Autism Bill to improve the lives of people with autism and their carers.
Carers provide unpaid care by looking after an ill, frail or disabled family member, friend or partner. There are 185,000 carers in Northern Ireland and every year another
69,000 people begin caring, many of whom do not know how to cope with their new and demanding role. This includes parents and others struggling to come to terms with the impact that autism has on a family, and on individuals living with autism.
Carers Northern Ireland is here to improve carers' lives.
- We fight for equality for carers. We want carers to have the same right as everyone else to an ordinary life – a fair level of income, adequate support to protect their health and wellbeing and access to the world of work, leisure and education
- We want carers to be recognised and actively involved as key partners in the design, delivery and provision of health and social care services.
Carers often contact Carers Northern Ireland's information and advice service when they have reached crisis point and do not know where to turn to for help. We help carers through the maze and give them:
- Advice on their rights so they can make important decisions about their lives
- Information about the practical help available to make caring easier
- Support by putting them in touch with other carers who understand the ups and downs of caring and can help ease their isolation and signpost to other local help
Carers give so much to society yet studies (including the Health & Social Wellbeing Survey and the NI Life and Times Survey) show that they are prone to poor health, stress, social isolation and poverty because of their caring role.
For most families, support from the wider family network is not forthcoming, so they are highly reliant for backup, information and support on the statutory services provided by Health & Social Care Trusts.
The Autism Bill
In responding to the proposals, we are conscious that opinion is divided amongst carers who are aware of the Bill, with some being strongly in favour of the legislation, and some who feel strongly that it is not worth the cost and effort involved.
Proposals relating to Autism Strategy
Our sense is that most carers are not particularly concerned about the detail of this or any other legislation – what they care about are the support and services they can access day to day.
Carers Northern Ireland is strongly in favour of concerted attempts to improve support for autism and to ensure consistent access to services and support across Northern Ireland. We therefore support an effective, properly implemented Autism Strategy.
We are not convinced, however, that legislation is required to put a strategy into place. There have already been a number of strategies developed within Health and Social Care to drive service improvements in Northern Ireland, including a Carers' Strategy. The content of these strategies is broadly similar to the contents proposed in the Bill and have been developed without the need for legislation.
Our experience is that the success of these rests on a number of factors: clarity of vision, buy-in at a senior enough level within the service, clear and achievable recommendations, effective monitoring arrangements and adequate resourcing. None of these factors require legislation.
Moreover, the Autism Spectrum Disorder Strategic Plan and the Regional ASD Network established in 2009 appears to offer an existing mechanism for achieving many of the objectives laid out in the Bill. It has already achieved considerable success in driving down waiting lists for diagnostic services. It may well be more effective to build on the work of this Strategic Action Plan and this Regional Network rather than to develop a new strategy which will no doubt cover much of the same ground. This may, in fact, delay implementation of much-needed positive changes on the ground.
Proposal to amend Disability Discrimination Act
Although it is undoubtedly true that carers are more concerned with the practical help they get than with the legislative basis on which it is provided, there is equally undoubtedly a real benefit to having clear and unambiguous rights in law.
Whereas we cannot see that a duty to develop a Strategy offers this benefit, there may well be benefit in amending the disability legislation to make absolutely clear the rights of people with autism to rely on the protections of the DDA.
The one concern that we would have is that, in refining the existing definition in the DDA, an attempt to improve access to legal rights and protections might inadvertently have the opposite effect. We could not hazard a legal opinion ourselves, but we would urge the committee to take legal advice from experts in the field of Equality that any amendment of the DDA will not have the consequence of excluding people with autism, particularly those with co-morbidity, from coming under the new definition.
Royal College of Speech and Language Therapists (RCSLT)
RCSLT Northern Ireland welcomes the opportunity to take part in this vital consultation. This response was formed following consultation with RCSLT Northern Ireland members who advise on, manage and deliver Autism services.
Royal College of Speech and Language Therapists
The Royal College of Speech and Language Therapists (RCSLT) is the professional body for speech and language therapists (SLTs), SLT students and support workers working in the UK.
The RCSLT has over 13,000 members, representing approximately 95% of the speech and language therapists working in the UK (registered with the Health Professions Council). We promote excellence in practice and influence health, education, care and justice policies.
Speech and language therapists play a major role in working directly with children and adults, as well as supporting other professionals in working with speech, language and communication needs.
Speech and language therapy as an early intervention for children plays a critical role in breaking the inter-generational cycle of poverty.
Communication Disability
Communication disability impairs the social and emotional capabilities of children and adults. It is the most common disorder seen in childhood, affecting up to 10% of all children (Law 2007).
Emerging research demonstrates that over 60% of children within the justice pathway have a communication disability, which is so severe that it prevents them from accessing prison educational programmes (Bryan et al 2007; Bryan et al 2004).
Prevalence of speech, language and communication difficulties.
- As many as 10% of children in the UK (over 1 million) have speech language and communication needs (SLCN) that require specialist help. This represents approximately three children in every classroom (Law 2000).
- Up to 55% of children in deprived areas experience speech and language difficulties at age five (Locke & Ginsborg J 2002). This figure includes children with the range of SLCN identified at birth or during pre-school, primary and secondary school.
- Over a quarter of all mainstream-educated, statemented children have speech, language and communication as their primary need.
- Two-thirds of 7-14 year olds with communication difficulties have additional behaviour problems (Cohen et al 1998).
- Over 60 % of young offenders have SLCN (Bryan et al 2007; Bryan et al 2004). Without intervention, SLCN impacts on literacy development, educational outcomes, emotional and social development. Children with SLCN are at an increased risk of emotional and behavioural difficulties (which are often misdiagnosed). Unsupported, approximately one third of children and young people with SLCN will go on to require treatment for mental health problems (Clegg, Hollis and Rutter 1999) and over two thirds will enter the justice system.
Commentary on Clauses
RCSLT NI makes the following comments in relation to the clauses as defined within the Autism Bill below.
Clause 1 - Amendment to the Disability Discrimination Act 1995
Clause 1 amends the Disability Discrimination Act 1995 ("the Act"), first by amending the definition of disability in the Act. Whereas the current definition of 'disability' makes reference to having "a physical or mental impairment", the present bill will amend the definition to include reference to 'social' impairments. Social impairments are to be interpreted as including communication difficulties.
1. - (1) The Disability Discrimination Act 1995 is amended in its application to Northern Ireland as follows.
(2) In section 1(1), after the words "a physical" insert ", social (including communication)";
(3) At the end of paragraph 4(1) of Schedule 1 insert —
"(i) taking part in normal social interaction; or
(j) forming social relationships."
RCSLT NI previously commented upon the definition of disability in the Disability Discrimination Act as it was felt at the time that the act would not sufficiently support the needs of individuals with communication disabilities.
RCSLT believe that the change in wording to the act proposed in this Bill will further discriminate against individuals with communication disability who do not have a social communication difficulty. The statement 'Social impairments are to be interpreted as including communication difficulties' may be misinterpreted as suggesting that all communication disabilities are subordinate to or result from social impairment. In fact many communication difficulties are not co morbid with Autism and will therefore still be excluded in this bill. RCSLT therefore recommends consideration of the following.
1. RCSLT propose further consideration of the current Disability Discrimination Act to review whether a social model of disability would be more inclusive. The current medical model can be viewed as being divisive as it may lead to discrimination by omission. RCSLT understands that there is support in NI for a review of this legislation by numerous voluntary bodies which support individuals with disability. This Autism Bill demonstrates that the current act is not fit for purpose and will continue to lead to concerns such as those rightly expressed by members of the Autism platforms.
The UN Convention on the Rights of Persons with Disabilities (CRPD) highlights the lack of inclusivity in our own disability legislation.
Article 21 Clause b 'Freedom of expression and opinion and access to information' states that society must enable 'accepting and facilitating the use of sign languages, Braille augmentative and alternative communication and all other accessible means modes and formats of communication of their choice by persons with disabilities in official interactions'. If the suggested amendment is made to the DDA it will still exclude individuals with a communication disability that is not the result of physical, sensory or mental disability.
|
A young man with a fluency difficulty (stammer) is more likely to suffer poor mental health, employment difficulties and reduced educational attainment. Half a million people in the UK stammer. Stammering is found in all parts of the world and affects the rich, the poor, those that are highly intelligent and those who have learning difficulties. Stammering is not simply a speech difficulty but is a serious communication problem. For the child or adult who stammers it can undermine their confidence and self-esteem, and affect their interactions with others as well as their education and employment prospects. It is a disability that is misunderstood and overlooked. |
2. If the Disability Discrimination Act is not reviewed RCSLT propose that the wording be changed as follows.
(2) In section 1(1), after the words "a physical" insert ", communication (including social communication)";
This would then reflect those in society who have a communication disability affecting any aspect of speech, language, voice, fluency (stammering), literacy or social communication.
Clause 1 also extends the definition of "normal day-to-day activities" in Schedule 1 (which supplements the definition of "disability" in the Act) so that a condition which has a substantial and long-term adverse effect on someone's ability to take part in normal social interaction or to form social relationships can constitute a "disability".
(3) At the end of paragraph 4(1) of Schedule 1 insert —
"(i) taking part in normal social interaction; or
(j) forming social relationships
RCSLT believe that it is not possible for this legislation to be so detailed in respect of what is considered normal social interaction or in forming social relationships and that this in itself does not constitute a disability for some individuals as it is part of their personality.
Clause 2 - Autism Strategy
RCSLT understand that significant investment and consideration of Autism is currently being supported by the DHSSPS and the HSCB. The Regional ASD Network (RASDN) is working to implement significant improvements to Autism services and RCSLT members are involved in this work and therefore do not support the need for a separate Autism Strategy. Members consider that this may lead to a duplication of existing resources and may cause considerable confusion for those participating in taking this current work programme forward. RCSLT would advise on consideration of an overarching 'communication strategy' which would encompass all individuals with a communication disability and would therefore be inclusive of individuals with Autism.
South Eastern Health and Social Care Trust
South Eastern Trust welcomes the opportunity to make a written submission in regards to the Autism Bill which has been referred to the Committee stage.
South Eastern Trust supports the general principles underpinning the Bill which is intended to have a positive impact on people with Autistic Spectrum conditions and aims to enable those with Autistic Spectrum conditions realise their full potential. The South Eastern Trust is of the view that specific legislation in this area is not required in addition to the existing legislation already in place. Any legislation introduced to address the needs of a specifically identified group, as in this case those on the Autistic Spectrum, runs the risk of highlighting the needs of one group of individuals over other groups who also have additional support needs.
The Trust would also be concerned that specific legislation could lead to an over emphasis on diagnosis rather than on meeting individual need and providing personalised care. The Trust's view is that individuals should be assessed on their needs not on a diagnostic label in keeping with a social rather than medical model of disability. Current legislation and policy places clear statutory duties on Trusts to assess each individual's unique circumstances with the service user and their carer central to the assessment process. The Trust would wish to avoid the development of a hierarchy of disabilities which would have the potential to create greater inequalities for other conditions not covered by specific legislation.
Clauses 1- 3;
The Trust recognises that any legislation needs to add value and make a real difference in comparison to what can be achieved without legislation. The Trust believes that appropriate legislation is already in place to ensure equity of access to services for individuals on the Autistic Spectrum.
Significant strides in the development of services for individuals with Autistic Spectrum Disorder have already been achieved, without specific legislation, through the independent review of Autism services, a regional Action Plan and investment funding over recent years. The establishment of the regional Autism Network, and associated regional project structure, has facilitated the development of a timeframe with specific recommendations for service improvement. Central to the process has been representation from service users and their carers and their involvement in service planning and monitoring service delivery.
With regards to Clause 2 (development of an Autism Strategy and collation of prevalence data) South Eastern Trust believes that the structure to deliver improvements are already in place through the regional A.S.D. network. In regards to data collation, South Eastern Trust is constantly working to improve data collation across both children's and adult services and view this as central to service development which does not require legislation.
Clause 3; South Eastern Trust recommends that the Content of the strategy must set out how the needs of people with Autism are to be addressed throughout their lives. Furthermore the focus should be on how services can be delivered that support individuals to maximise their independence throughout their lives rather than focus on how needs are to be addressed which may convey dependency and undermine independence.
In terms of training the Trust would support the need for targeted awareness training and would refer to the progress made by the regional network in this area.
The Trust remains committed to improving Health and social care services for children and adults with Autistic Spectrum conditions and for those who care for them. The Trust will continue to lead the local A.S.D. forum to maintain a multi- agency focus on service development in the South Eastern Trust area.
I hope you find this helpful and please do not hesitate to contact me should you require any further information.
Mencap
1.0 About Mencap
Mencap is a voluntary organisation which works alongside and represents the views and interests of people with a learning disability and their families. We provide a range of services to children, young people, men and women with a learning disability and their families throughout Northern Ireland. Our services and activities support people across the spectrum of learning disability, including individuals with autism. We support a membership network of over 50 local groups, including Gateway Clubs, and campaign for equal rights and opportunities for everyone with a learning disability.
Our vision is of a world were people with a learning disability are valued equally, listened to and included.
2.0 Support and services for people with autism and their families
Mencap recognises that, for too long, people with autism and their families have not been getting support and services to meet their needs. We recognise, too, the failure of departments and other public bodies to adequately address the inequalities experienced by people with autism, including people with a learning disability who also have autism. We agree that the needs of people with autism, including people with a learning disability, are not properly understood or planned for and that much needs to be done to address the myriad barriers they face and which result from structural and commissioning arrangements, restrictive eligibility criteria and inadequate levels of resourcing. We agree, too, that the difficulties and barriers between and within departments and other public bodies need to be addressed and better, more robust mechanisms developed to strengthen joint planning, funding and monitoring arrangements.
3.0 The Autism Bill (NI)
Mencap understands the importance of legislation in ensuring that people are able to access the support and services they need and should be entitled to. We believe, however, that legislation should promote fairness rather than result in inequalities between people who have a similar need for support. We believe that legislation should give a guaranteed access to support and services based on the needs of an individual rather than based on a clinical diagnosis.
4.0 Conclusion
Mencap welcomed the opportunity to comment on the proposals outlined in the consultation paper.
The Royal College of General Practitioners in Northern Ireland
The Royal College of General Practitioners in Northern Ireland (RCGP) is grateful for the opportunity to comment on the Autism Bill and proposed Autism Strategy.
The Royal College of General Practitioners in Northern Ireland has over 1,200 local GPs as members, which accounts for over 80% of all GPs in Northern Ireland. Our membership includes GPs from a range of work areas including registrars, locum GPs, trainers, tutors and academic GPs. The Royal College of General Practitioners is an international organisation with over 40,000 members worldwide, making us the largest Royal College within the United Kingdom.
As a registered charity we place the needs and care of patients at the centre of our work. Our aim is to encourage and maintain the highest standards of general medical practice and act as the 'voice' of General Practitioners on education, training and issues about standards of care for patients.
Response
The RCGP Northern Ireland (NI) is grateful for the opportunity General Practitioners are in a prime position to witness the effects of autism on the lives of patients' and their families/carers and the RCGP NI welcomes the publicity that the debate surrounding the bill has brought to this condition.
RCGP NI is aware of the current Autism Act 2009 in England and the subsequent Autism Strategy in England.
Accurate information regarding autism diagnosis, prevalence, management, and support in Northern Ireland is needed and any strategy adequately addressing this would be welcome.
The resource required to address this particular area of disability adequately would be considerable but without a specific review of the current position for autistic spectrum disorder in Northern Ireland it is difficult to proceed with any plan for the future. Although the resource implications for such a strategy are expansive, that itself, should not deny sufferers of this condition the opportunity to have their care and support assessed.
Any strategy would however have to include provision of relevant services for the purposes of diagnosing autistic spectrum conditions in the adult population as well as in childhood and the range of symptoms and variation in severity of manifestation brings ambitious challenges. However within the boundaries of current resources, adults and children with autism should be able to seek help on a level playing field with other disability groups.
With regard to changes to the wording of the Disability Discrimination Act 1995, it is not clear that this is necessary and in fact could lead to confusion over the definition and interpretation of the term "social" with regards to disability.
In England in October 2010 the Disability Discrimination Act 1995 was replaced by the Equality Act 2010. The Equality Act defines a person with a disability if they have a physical or mental impairment, and the impairment has a substantial and long-term adverse effect on the person's ability to carry out normal day-to-day activities. The Act does not include the word "social" in its definition.
The Autism Act in England was set up before the implementation of the Equality Act, i.e. under the Disability Discrimination Act 1995. The Autism Act makes no mention of the term "social disability". The act placed a duty on the Secretary of State to prepare and publish an autism strategy in England.
Within the English Autism Strategy which arose from the Autism Act, autism is defined as a lifelong condition that affects how a person communicates with, and relates to, other people and lists three main areas of difficulty: social communication, social interaction and social imagination. The strategy makes no mention of the term "social disability".
Inserting the word "social" into section (1) of the Disability Discrimination Act 1995 is not needed to accept autism as a disability. Autism is a complex developmental disability affecting psychological and behavioural development and is not defined as a "social" disability.
Northern Health and Social Care Trust
General comment
This Trust is aware that opinions on the proposed legislation are still very much split and this will require an informed and reasonable discussion at Committee Stage. Some argue that the Disability Discrimination Act is more than effective as it presently sits, regarding those who have a diagnosis of autism spectrum disorder. Specific legislation is not under consideration and therefore ask the reasons why autism should be treated differently.
It is also recognised that there has been a historical lack of strategic planning and joined up working, and there are individuals with ASD who are unable to access needed services which specific legislation could help address. However, careful consideration needs also to be given as to whether these issues could be addressed within the framework of existing children's and disability discrimination legislation or whether this could only be achieved through the proposed legislation.
The current ongoing work undertaken by RASDN has, in developing an action plan, allied to targets, begun to impact on awareness across the region, as have recent Judicial Review decisions made under existing legislation.
There is acknowledgement of the need for change, and a recognition that, legislation or not, a vision and related guidance are required in terms of how the needs of families and carers are to be addressed.
Specific Comment
Clause 1
There is no issue with amendment to social impairment. With regard to 'normal day to day activities' we would suggest an insertion about vulnerability as a result of inappropriate social interaction.
Clause 2
With reference to the department seeking information from five Trusts prevalence, this is particularly difficult within adult services as many ASD people are coded on IT systems with regard to the service/therapy/treatment they are getting and not on an autism coding. There are clearly IT implications with this issue.
Clause 3
The view here is that for adults, the strategy would only refer to people with a diagnosis of ASD and an associated social dysfunction.
National Autistic Society Northern Ireland
The National Autistic Society (NAS) Northern Ireland is the charity working throughout Northern Ireland for people affected by autism. In Northern Ireland we provide information, advice and support and campaign and lobby for lasting positive change for those affected by autism. We have twelve NAS branches in Northern Ireland, providing local sources of information and support.
NAS Northern Ireland delivers a number of services including:
- Our help! Programme which provides parents and carers of school-age children, young people and adults with post-diagnostic information, advice and support
- Our Befriending scheme which trains and supports volunteer befrienders to spend a few hours a week with an adult or child with autism or Aspergers syndrome or a family member
- Parent to Parent confidential telephone support service, provided by trained parent volunteers who have personal experience of autism and want to support other parents
- Our telephone based Advocacy for Education service, which provides information, advice and support on education provision and entitlements to help guide families through education law
- Support group for parents of adult children.
- Teenscene for young adolescents
- Our Social Groups are for over 16's with high functioning autism or Aspergers syndrome and meet once a month for social activities.
- Our team of family support workers who act as advocates for parents providing practical and emotional support.
- A range of social and leisure activities for children and adults with autism.
What is an autism spectrum disorder?
Autism is a lifelong developmental disability that affects the way a person communicates with, and relates to, other people. It also affects how they make sense of the world around them. It is a spectrum condition, which means that, while all people with autism share three main areas of difficulty, their condition will affect them in different ways. The three main areas of difficulty (sometimes known as the 'triad of impairments'[1]) are:
- Difficulty with social interaction. This includes recognising and understanding other people's feelings and managing their own. Not understanding how to interact with other people can make it hard to form friendships.
- Difficulty with social communication. This includes using and understanding verbal and non-verbal language, such as gestures, facial expressions and tone of voice.
- Difficulty with social imagination. This includes the ability to understand and predict other people's intentions and behaviour and to imagine situations outside of their own routine. This can be accompanied by a narrow repetitive range of activities.
Some people with autism are able to live relatively independent lives but others may need a lifetime of specialist care. People with autism may also experience some form of sensory sensitivity or under-sensitivity, for example to sounds, touch, tastes, smells, light or colours.
Asperger syndrome is a form of autism. People with Asperger syndrome are often of average or above average intelligence. They have fewer problems with speech but may still have difficulties with understanding and processing language. People with Asperger syndrome may not necessarily have learning disabilities but often have accompanying learning difficulties, including dyslexia.
We use the term autism here to cover all people on the autism spectrum, including autism, Asperger syndrome and other diagnostic terms used for autism spectrum conditions. Over 17,000 people in Northern Ireland have autism if you count their families autism touches the lives of over 68,000 people. Despite this, autism is still relatively unknown and misunderstood. That means that many people affected by autism and their families get nothing like the level of help, support and understanding they need.
Overview of the involvement of the National Autistic Society in the Development of autism initiatives in England, Scotland, Wales and Northern Ireland
The National Autistic Society was one of the principal proponents of the Autism Bill which became the Autism Act in England in 2009. We worked with 13 other autism organisations to take this forward. This resulted in the development of an Adult Autism Strategy in March 2010. Statutory Guidance for local authorities and health bodies is currently being consulted on.
In Scotland the National Autistic Society has pioneered an Autism Bill which is currently in the Scottish Parliament.
In Wales the National Autistic Society has been active in the development of the Autism Spectrum Disorder Strategic Action plan which sets out how services will be delivered to people affected by autism in Wales.
In Northern Ireland the National Autistic Society has been an active member of the Regional Autistic Spectrum Disorder Network (RASDN) which was formed to take forward the DHSSPS ASD Strategic Action Plan. The National Autistic Society Northern Ireland sits on the Reference Group, the adult subgroup, communications group and the Northern Trust ASD forum. We are also involved in the Transitions, Interventions and Training work streams.
Autism Bill NI
Background and policy Objectives
The National Autistic Society Northern Ireland supports the main objective of the Autism Bill which is to enhance the provision of services to and support for people with Autistic Spectrum Disorders
Clause 2 the Autism Strategy
The National Autistic Society Northern Ireland supports clause 2 of the Autism bill which requires all Northern Ireland Government Departments to co-operate in the development of an autism strategy and to implement any part of the strategy for which they are responsible.
Amendment to the Autism NI Bill
Whilst the National Autistic Society Northern Ireland welcomes the intention for consultation between NI government departments we are concerned that the depth of knowledge and experience of people affected by autism and their parents/ carers and the voluntary sector will not be sufficiently considered if not outlined in the Bill. The National Autistic Society Northern Ireland suggests an amendment to the Bill which will outline their involvement in the process. The proposed amendment could be inserted in Clause 2 on page 1
- The Department should establish a reference group comprised of people with autism, parents/carers, and representatives from the voluntary and statutory sector to develop the autism strategy and to oversee its implementation.
Clause 3 – Content of the Autism Strategy
Whole life support for people with autism
The National Autistic Society Northern Ireland supports the content of the strategy in relation to requiring the lead Department to set out how the needs of people with Autistic Spectrum Disorders are to be addressed throughout their lives. Health and Social Care has started to address some of the historic deficiencies in the Health and Social Care sector in relation to autism. In June 2009 Minister Michael McGimpsey published the ASD Strategic Action Plan which arose out of the independent review of autism services which was chaired by Lord Maginnis.
The Minister commissioned the Regional Autistic Spectrum Disorder Network to take forward the implementation of the Strategy. Dr Bergin and Lord Maginnis head up this process. This has started to produce results.
Why we Need a Cross Departmental Strategy for Autism
Below is a brief synopsis of current initiatives in relation to Autism and also an outline of areas that the National Autistic Society Northern Ireland believes would benefit from cross-departmental working.
Health and Social Care
Work of RASDN
The National Autistic Society Northern Ireland is an active participant of the Regional Autistic Spectrum Disorder Network (RASDN). What is unique about RASDN is the involvement of parent/carers, people with autism, the voluntary sector and the statutory sector who are all working together to devise services that best meet the needs of people with autism and their families and carers. Parents and carers are officially mandated as advisors to the Reference Group and to each Trust. They are involved in all recent investments and in service improvement. RASDN is working well and we are starting to see outcomes from the Group
Some of the outcomes of the group include;
- Financial Investment in Autism Services £1.54 million over the 2009 -2011 an extra 100k announced (November 2010) which brings the recurrent total new investment to 1.64m from April 2011
- Development of the children's diagnostic pathway which will be implemented across all Trust areas
- A reduction in waiting lists re assessment to 13 weeks (four of the five trusts are now meeting this target. All Trusts should be compliant by March 2011.
- The recommendations for the Adult Diagnostic pathway will be available in January 2011
- Work streams are ongoing in Training, Interventions and Transitions
- Information resource to guide parents/carers and people with autism to relevant services and resources throughout their life.
The National Autistic Society Northern Ireland supports the work of this group and would suggest that any future strategy needs to ensure that this work is continued.
The National Autistic Society Northern Ireland recommends that any future strategy that arises from the Autism Bill should adopt the structure of RASDN (i.e. ensuring that parents, carers and people with autism the voluntary sector and the statutory sector are all actively involved in service design, improvement and investment). As outlined previously we have suggested an amendment to the Autism Bill to facilitate this.
RASDN is producing results in Health and Social Care but it does not have a remit over education or Employment and Learning although education is represented on the reference group..
Education
The Department of Education is working on the production of an education strategy for children with autism. Recent proposed changes outlined in the SEN Review resulted in an unprecedented number of responses from concerned parents, many of whom where parents of children with autism. While the National Autistic Society Northern Ireland supports the production of an Education Strategy for children with autism we believe that it needs to work in tandem with the Department of Health and Social Services and the Department of Employment and Learning. We also believe that an Education Autism Strategy should be produced in conjunction with the voluntary sector and parents, carers and people with autism in the same way that RASDN works.
Education must ensure that the needs of children with autism are met; children with autism need specialised autism specific support if the best outcomes are to be achieved. Below a parent of a child with autism outlines her experience of the complexity of the condition and the need to provide specialised, well resourced support. It is a lack of resources which prevents the employment of a 1:1 assistant in this case.
|
"My son is generally in good health. His language is reasonably good and he has a good vocabulary. However, he repeats the same things over and over again and insists that you listen intently. He has reasonably good relationships with family members but his unpredictable behaviour makes it difficult for him to sleep over with all but the closest family. He is very sociable but often approaches strangers. He seems to persevere with school more than enjoy it. He refuses to go to school at least twice a week and does not talk about his activities unless pressed. School have identified him as an excellent candidate for 1:1 support which they are unable to provide. His work is cut down so I believe that he is not accessing the full curriculum He is a frustrated child. He does not understand why certain behaviours are not acceptable or are inappropriate. He has regular tantrums when things do not go his way. His behaviour is very unpredictable and going out always has the possibility of being cancelled if he puts himself or one of his siblings in physical danger. He tries very hard to follow rules but is regularly disappointed when he doesn't manage it. Our main concern is that without support and assistance, he will never achieve his potential whatever that might be and that his mental state will continue to deteriorate as his peers move further and further away educationally." |
Calls from parents to our Education helpline are often on the issue of what parents feel is a lack of understanding of ASD and the provision of specialist support. Below is a quote from a Parent outlining her experience of how a school has addressed the issue of autism.
|
"A number of incidents have happened since the start of term. The school has dealt with these simply as incidents of bad behaviour. I feel that the problems are due to sensory issues which have not yet been understood or addressed. My son is beginning to say that he "hates school" and I am beginning to lose confidence in the school. I am starting to consider educating him at home" |
The quote below outlines the difference that appropriate specialised support can make to a child with autism.
|
My son's educational needs are best met in a highly structured environment. The support he has received so far illustrates that his needs require a predictable, understanding environment. For reasons of health and safety and to enable my son to develop, he will require constant 1:1 adult support and supervision. The benefits of having support from adults with a good knowledge of autism spectrum disorders has been proven and is very obvious to us as parents. |
The National Autistic Society Northern Ireland believes that education plays a fundamental role in addressing the needs of children and young people with autism. To ensure effective intervention Education needs to develop its Strategy in conjunction with The Department for Health and Social Care and the Department for Employment and Learning. Children with autism often need to avail of Speech and Language and OT therapies within the school environment and these are often outlined on a child's Statement of Special Educational Needs, however there is no legal obligation for the Department of Health to provide these services.
Adults with Autism
Any Strategy that is produced must pay particular attention to the issue of adults with autism. The National Autistic Society Northern Ireland's I Exist research found that Adults with autism are often unable to access the right support, and consequently often become dependent on their families. 75% of adults with autism rely on their families for financial support; only 13% live independently. 96% of the adults who took part in our research felt that with more support they would feel less isolated. As a direct result of this lack of support 34% of adults in our survey have experienced severe mental health difficulties and 57% suffered from depression. There has been a historic lack of funding for services for adults with autism and this needs to be addressed
Adults with autism also experience issues with regards to accessing employment and benefits.
Employment and Benefits
In October 2009 the National Autistic Society launched its Don't Write Me Off Campaign which aimed to make the system for accessing employment and benefits fairer for adults with autism. The report for the campaign surveyed a group of adults with autism across the UK and found that:
- One third are currently without a job or access to benefits
- Over half have spent time with neither a job not access to benefits, some for over ten years
- Just 15% have a full time job
- 79% of those on Incapacity Benefit want to work
- 82% who have applied for benefits say they needed support to apply
In order to address the needs of adults with autism more needs to be done to ensure that adults with autism are able to get a job when they can work and benefits when they can't.
Awareness of Autism in Northern Ireland
The National Autistic Society Northern Ireland supports the inclusion within the Bill of an awareness raising campaign on autism. As part of the research for the I Exist campaign the National Autistic Society Northern Ireland commissioned a leading market research company to survey a sample of 500 people aged 16 and over across six counties in Northern Ireland. We asked our respondents what proportion of the population they thought were affected by autism. The vast majority 90% did not know how common autism was. Our survey revealed that 87% of the population have heard of autism but far fewer only 48% had heard of Asperger syndrome. There was also considerable confusion about the nature of autism for example 62% of our respondents believed that people with autism have special abilities for example in maths or art. Widespread misconceptions make it difficult for people with autism to get the right kind of support.
Resources
The main challenge to the work of RASDN or to the cross departmental strategy as outlined in the Bill is Finance. The historic underfunding of autism services needs to be addressed. The Minister has made resources available for autism which we welcome but more is urgently needed if we are to meet the needs of people with autism and their families and carers. This is particularly relevant in relation to the development of services for adults with autism. In the present economic climate this will be challenging.
In an analysis of the economic costs of autism in the UK Martin Knapp concluded [2]"If early intervention could successfully change some aspects of behaviour that are cost-raising, both in childhood and subsequently, it may allow cost savings to be made and quality of life improvements to be achieved.
[1] Wing, L. and Gould, J. (1979) Severe impairments of social interaction and associated abnormalities in children: epidemiology and classification. Journal of Autism and Developmental Disorders, Vol. 9(1), pp. 11-29
[2] Martin Knapp, Renée Romeo and Jennifer Beecham (2009) Economic cost of autism in the UK, Autism 13: 317-337
http://www2.lse.ac.uk/ERD/pressAndInformationOffice/newsAndEvents/archives/2009/05/MartinKnappAutism.aspx
Department of Enterprise, Trade and Investment
Disability Action
Department of Finance and Personnel
Belfast Health and Social Care Trust
In its response to the Autism Bill (NI) consultation the Belfast Trust welcomed a raised profile for people with autism and emphasised its commitment to seek improved opportunities for people with all disabilities. Within this context the Trust raised some concern that legislation focusing on one single disability could be perceived as disadvantaging those with other disabilities. The Trust remains concerned that a Bill focused purely on ASD will create a "hierarchy" of disability. It may also create confusion for people for whom ASD co-exists with another condition. Recent evidence would indicate that a significant proportion of people on the ASD spectrum have co-morbid disabilities. The Trust would not wish to see disputes arising over which disability took precedence and which are covered by legislation.
In relation to the specific Clauses of the Bill the Trust wishes to comment as follows:-
Amendment to the Disability Discrimination Act 1995 (c. 50)
The Trust is committed to equality for all those with disabilities and therefore welcomes the proposed specific references to social (including communication) and also particular mention of social interaction and social relationships within this context. The Trust is of the view however, that legislation in N Ireland already has comprehensive provision particularly for children in need, which includes those with ASD. The Children Order 1995, The Disability Discrimination Act 1995 and the Children's Services Planning Order 1998 already place significant responsibilities on Trusts for the assessment and provision of services for those in need. Much of the strategic development in N Ireland has been underpinned by the UN Convention on the Rights of the Child and the UN Convention on the Rights of Persons with Disabilities. Both Conventions make it clear that provision of services should be made based on assessment of need. A Bill which uses a model of provision based on medical diagnosis is not in keeping with these well respected Conventions and makes a shift away from the accepted social model of disability.
Autism Strategy
The Trust welcomes the emphasis placed on an interdepartmental approach to the preparation and implementation of this proposed Strategy as this reflects the essential requirement of a multi-disciplinary and interagency approach to meeting the needs of this group. The Trust has welcomed the existing ASD Strategy and is an active member of the Regional Network. The Trust takes the view that the leadership provided through that Network is already making excellent progress in the areas required. It is difficult to see what added value would be brought to this work by a legislative framework. It is noted that there is no specific reference in this section to consultation with the voluntary and community sectors which currently provide a range of valuable services to families and it may be appropriate to review this omission. The existing ASD Strategy puts families and voluntary sector partners right at the heart of the Network.
In relation to preparation and availability of data it should be noted that the requirements of the proposed Bill will have to be accompanied by more robust systems of data collection by all departments providing services particularly in instances of co-morbidity. Within this context it should also be noted that autism as a developmental condition can take differing timescales to diagnose and this may also impact on data collection. The Trust would be concerned that legislation could result in improvements in data collection for people with ASD at the expense of improved data collection and information systems for people with other disabilities such as Down's Syndrome or Cerebral Palsy.
Content of the Autism Strategy
The Trust welcomes the specific reference to the "Health Care, Educational and Social Needs" of persons with autism and is acutely aware of the critical interface with schools and Education & Library Boards particularly in meeting the needs of children and young people. The Trust also welcomes the focus on meeting the needs of both persons with autism and also their families and carers. Within this context the Trust is mindful of the relative underinvestment in services for disabled persons and current budgetary constraints and considers it essential that appropriate cognizance is given to the resource issues accompanying additional statutory responsibilities and public awareness.
Interpretation
The Trust notes the definition of "Autism" provided under Section 4 and in particular the inclusion of "any pervasive development disorder not otherwise specified". In relation to carers the Trust considers that it may be helpful to provide some guidance in relation to the definition of "substantial" as it relates to the amount of care provided.
As outlined above Belfast Trust has significant concerns that such a Bill will result in ASD becoming a "more important" condition than other disabilities. Nevertheless should the Bill be ratified, the Trust will play its full part in implementing any new recommendations.
Regional Autistic Spectrum Disorder Reference Group
Amendment to the Disability Discrimination Act 1995
Amendment to the Disability Discrimination Act 1995 (c. 50)
1.—(1) The Disability Discrimination Act 1995 is amended in its application to Northern Ireland as follows.
(2) In section 1(1), after the words "a physical" insert ", social (including communication)";
(1) Subject to the provisions of Schedule 1, a person has a disability for the purposes of this Act if he has a physical, social (including communication) or mental impairment which has a substantial and long-term adverse effect on his ability to carry out normal day-to-day activities.
(2)In this Act "disabled person" means a person who has a disability. (DDA 1995
(3) At the end of paragraph 4(1) of Schedule 1 insert¾
"(i) taking part in normal social interaction; or
(j) forming social relationships."
4(1)An impairment is to be taken to affect the ability of the person concerned to carry out normal day-to-day activities only if it affects one of the following—
(a)mobility;
(b)manual dexterity;
(c)physical co-ordination;
(d)continence;
(e)ability to lift, carry or otherwise move everyday objects;
(f)speech, hearing or eyesight;
(g)memory or ability to concentrate, learn or understand; or
(h)perception of the risk of physical danger.
(i)taking part in normal social interaction; or
(j)forming social relationships.
(DDA 1995
Insofar as the (inserted in purple above) relevant extract from the Disability Discrimination Act 1995 in concerned one can see what is being attempted BUT the argument is flawed – not least in that only OFMDFM has competence in relation to the DDA 1995.
While one can define medically physical and mental – how does one define 'social' – what is 'social' … indeed what is normal? Is it refusal to take part in the church choir; to play rough sport; to participate in hare-coursing or to go down to the pub with the lads? To use this term is to create a 'silo' where individuality, personal prejudices and choices must be subjected to scrutiny. 'Social' identifies society, but society varies according to so many things e.g. the guy who makes frequent use of the 'f' word is normal in some circles and could be a virtual outcast in others.
To seek to define Autism Spectrum Disorder exclusively in terms of it being a 'social disorder', as this Bill does, would actually eliminate many on the spectrum who need interventions and support.
Whatever this Bill is intended to do - and at no point is that clear – it is drafted to be exclusive, not inclusive, in relation to those on the spectrum.
(Purely for compatible drafting and grammatical consistency (i) should read 'social interaction' and (h) 'social relationships'.)
For much of the Bill the word 'Department' appears undefined – in fact it is eventually found in 4(1) to be the DHSSPSNI. What are the implications of this?
The Autism Strategy
Autism strategy
2.—(1) The Department must prepare a strategy on autism to be known as the autism strategy and must publish the autism strategy not less than two years after the passing of this Act. The Department has already carried out an Independent Review of Autism Services and is a year into implementing the Review's recommendations. It is, literally, involving parents, carers and users at Trust level in all aspects of service provision including 'commissioning'. Should this work be suspended for 2/3 years to facilitate the Bill.
(2) Before preparing the autism strategy, the Department must consult the Northern Ireland departments on it. This means the disempowerment of Parents, Carers and Users – it would be retrograde – a bureaucratic exercise involving groups of Civil Servants (who would initially have to be brought up to a standard of specialisation) taking literally years – anyway other Departments will not be willing to be subservient to Health.
(3) The Department must request every HSC trust to provide data on the prevalence of autism in its area in order¾
(a) that it can publish and update the strategy; and
(b) that the Northern Ireland departments can effectively implement the strategy. This is inherent in the current implementation of the Independent Review's Recommendations and is already happening.
(4) The HSC trusts must provide the Department with all information it requests under subsection (3). Already in place among professionals.
(5) The Department must keep the autism strategy under review and must publish a revised strategy at intervals of not more than seven years. Why 7 years – effective reviewing is professionally in-built – it should be seamless development and not some sort of staging post.
(6) The Department must monitor the implementation of the autism strategy by the Northern Ireland departments. Again, Departments co-operate but one cannot be 'bossed' by another.
(7) The Northern Ireland departments must co-operate with the Department in relation to the preparation, review and implementation of the autism strategy. This is currently being done by consultation, with Parents, Carers & Users who form the N.I. Regional ASD Reference Group being consulted and directly involved at both Trusts and Departmental level. (see note on Autism N.I. below).
(8) The Northern Ireland departments must implement that part of the autism strategy which falls within their responsibilities and the Department must implement that part of the autism strategy which falls within its responsibilities. Don't need an act to state the obvious – but it's done by co-operation – not by diktat.
(9) Not more than three years after the publication of the autism strategy, and at intervals of no more than three years thereafter, the Department must prepare a report on implementation of the autism strategy by the Northern Ireland departments and the Department. Once again Health simply do not and cannot speak for or have the dominance over other Departments that this would require.
(10) The Minister shall lay a report prepared by the Department under subsection (9) before the Assembly as soon as possible after its preparation.
Content of the autism strategy
3.—(1) The autism strategy must set out how the needs of persons with autism are to be addressed throughout their lives.
(2) Without prejudice to the generality of subsection (1) the needs to be set out in the autism strategy shall include the health care, educational and social needs of persons with autism. This Bill is flawed insofar as it fails to address individual Departments' responsibilities – this Bill would impose on Health responsibilities outside its bailiwick.
(3) The autism strategy must set out how the needs of families and carers of persons with autism are to be addressed. Now what does this mean – again it appears that e.g. benefits somehow all fall within the scope of Health – it becomes more ridiculous insofar as it suggests a one size fits all policy – currently the Reference Group in looking at how one provides individual pathways.
(4) The autism strategy must set out the Department's proposals for promoting an autism awareness campaign.
(5) The autism strategy must set out the steps the Department proposes to take to ensure that public servants who deal directly with the public in the course of their duties are given autism awareness training. Everyone including bus drivers, taximen and shop assistants? Seems like this is DELNI's Area of Responsibility – the Reference Group is already engaged in this exercise.
(6) The Department may make regulations as regards the content of the autism strategy.
3 above has already a multiplicity of sources of information; ongoing research and practical aspects to be implemented. "Within a year we have had every Health Visitor 'uptrained' so that every child of 2 years old can have a home visit to assess developmental progress (early identification); for those identified the waiting time for Assessment and Diagnosis will soon be down to 13 weeks in all Boards (4 Boards by Dec 'this year and the last by May '11); and interventions will be in place by 13 weeks after that. When I began the Independent Review there was an official waiting list of "387 waiting up to 35 months",
The difference in the current strategy is that it is being shaped by the Parents, Carers and Users themselves in direct consultation with the professionals – not dictated from Knockbracken by a Charity that is little more than a business selling services and with a CEO who believes she has a 'Right' to dictate from a detached 'ivory tower'– i.e. who claims virtusal 'ownership' of all the 20,000 who are on the spectrum but has no tangible 'on the ground' role. Remember the sponsors (or is it sponsor) of this Bill originally wanted to create a £100,000 per annum "Autism Advocate" post for someone.
Supplementary
Interpretation
4.—(1) In this Act, unless the context otherwise requires—
"autism" means autism, Asperger's syndrome, Rett's syndrome, Heller's syndrome or any pervasive developmental disorder not otherwise specified; Well! Very scientific – Autism is a 'catch-all!!
"autism strategy" means the strategy required to be published under section 2; So 'strategy' means 'strategy' – very enlightening !!!
"carer", in relation to a person with autism, means an individual who provides a substantial amount of care on a regular basis for that person;
"Department" means the Department of Health, Social Services and Public Safety; So now we know – ridiculous - but, implicitly, the DHSSPS will have superiority over all other Depts including OFMDFM?
"HSC trust" refers to a body established under Article 10 of the Health and Personal Social Services (Northern Ireland) Order 1991 (NI 1);
"Minister" means the Minister of Health, Social Services and Public Safety;
"Northern Ireland department" means the Department of Culture, Arts and Leisure, the Department of Education, the Department for Employment and Learning, the Department of Agriculture and Rural Development, the Department of Enterprise, Trade and Investment, the Department of the Environment, the Department of Finance and Personnel, the Department of Justice, the Department for Regional Development, the Department for Social Development and the Office of the First Minister and deputy First Minister; Pure nonsense – devoid of rationality and logic – 'department' now officially means 'Departments'.
"public authority" means a body established or constituted by or under a statutory provision;
"public servant" means an officer or servant of the Crown or of any public authority.
Regulations and orders made under this Act
5.—(1) No order or regulation may be made under this Act unless a draft of the order or regulation has been laid before, and approved by resolution of, the Assembly. Obviously this is the weakest element – basically no-one can actually show initiative unless the Assembly so permits – makes it more convenient for someone handily ensconced in Knockbracken to dictate the way forward – AND WHERE THE MONEY GOES!!!
(2) Before making a regulation or an order under this Act the Department must consult the Northern Ireland departments and such other persons as the Department thinks appropriate. Advocates a consultation procedure simply for the sake of adding the word "Social" - Sounds like 'manyana' to me – politicians to be led by Arlene Cassidy and to blazes with the professionals and consumers!!! Is Eileen Bell a paid lobbyist?
Commencement
6. This Act comes into operation after the end of the period of three months beginning with the day on which it is passed.
Short title
This Act may cited as the Autism Act (Northern Ireland) 2010.
This Bill would be a hindrance to initiative, professionalism and progress. Already any Department finding itself 'short' of a legislative provision is quickly and easily able to amend an appropriate current Act – Health has made huge strides without needing to do so. This Draft Bill is an aberration.
Department of Education
Introduction
This paper has been prepared in response to a request from the Committee for Health, Social Services and Public Safety for a briefing paper on the Autism Bill. It seeks to describe the type of support for pupils on the autism spectrum which was put in place following the publication of the Report of the Task Group on Autism in 2002 and to provide information on the current legislative base, which defines the statutory responsibilities of the Education and Library Boards (ELBs) and schools. Information is also provided on the progress of the development of an autism strategy and implementation plan for the education sector.
Contents:
1. Current Education Provision (including case studies)
2. Current Legislative Base
3. Special Educational Needs and ASD Statistics and Prevalence
4. Educational Resources for ASD and SEN
5. Task Group Report on Autism
6. ETI Report – An Evaluation of the Inter-Board ASD Advisory Service
7. DE Autism Strategy and Implementation Plan
1. Current Education Provision
1.1 Autism support is tailored to meet the needs of the individual pupil. The Code of Practice on the Identification and Assessment of Special Educational Needs (SEN) provides guidance to the Education and Library Boards and the boards of governors of the grant-aided schools (and those who help them including the health and social services) on their statutory duties. The Code sets out a 5 stage approach. School based support is provided at Stages 1 and 2 and at Stages 3, 4 and 5, individual pupil support may also be accessed and a more intensive level of support provided, which is based on the learning needs of the child.
1.2 Case Studies
Three theoretical examples of support for pupils with autism are detailed below, outlining the likely education provision that would be delivered under the existing framework for educational provision for those children and young people on the autism spectrum. Each example refers to children at different stages on the Code of Practice.
Case Study 1
Nursery aged child at Stage 1 of the Code of Practice with no confirmed diagnosis of ASD
Likely Support:
- Teacher support – school visits to discuss teacher concerns
- Training in ASD - whole school training and early years in-service training would be made available
- Following teacher consultation – specialist resources provided for the classroom e.g. schedules and positive behaviour visuals.
- Follow up school visits and telephone calls.
- On parental request, parent support, telephone contact and home visits would be available.
- Areas of concern identified would be within the home and advice and resources provided to home. Parents informed of other support services available e.g. Health and Social Services Trust.
Case Study 2
P7 pupil with a diagnosis of Autism
Likely Support:
- School based observations would inform tailored individual support
- Parent and teacher interviews
- School and home based resources would be provided
- Assistance would be provided to school with individual education plan
- Primary in-service training and whole-school training would be provided to school staff
- Liaison with educational psychology, occupational therapy and speech & language services
- Collaborative working with Health Board's Autism Service
- "Social Skills Workshops" for P7 pupil and parent (5 consecutive sessions)
- "Transfer Workshop" to prepare P7 pupil and parents for transfer to post- primary school environment and staff and parent completion of "Individual Pupil Profile"
- Autism awareness peer training for schools via Key Stage 1 and Key Stage 2 "Autism Awareness Puppet Shows"
- Buddy system and social group would be set up in school
- Explicit teaching of social skills – one to one and group level.
- Ongoing parental involvement to ensure continuity and generalisation of skills
- Contribute to transfer review advice, as part of the SEN process
Case Study 3
Year 10 pupil with a diagnosis of Asperger's Syndrome and associated behavioural concerns.
Likely Support:
- School based observations
- Parent and teacher interviews
- Liaison with other agencies involvement: - Child and Family Clinic (CFC), Child and Adolescent Mental Health Service (CAMHS), educational psychology and education welfare services
- Functional assessment and establishment of a school and home based "Positive Behaviour Support Programme"
- Appropriate risk assessment would be undertaken
- Supporting school staff in setting of autism-specific targets on education plan
- Working with student on setting appropriate social and behaviour targets and monitoring, evaluating and recording progress via daily target diary
- Explaining diagnosis of ASD to the parents and to the pupil
- "Autism Awareness Training Workshop" delivered to peers
- Pupil participation in five week "Anger Management Programme"
- Parental attendance at five week "Life Skills course for parents of Year 10 pupils with a diagnosis of ASD"
- Staff attendance at nine week course on "Supporting the pupil with ASD using the principles of Applied Behaviour Analysis"
- Post-primary in-service training and whole-school training would be provided to school staff.
Further training support can also be provided through to school staff, teachers, non-teaching staff and parents. This support may be accessed directly by schools and parents from the Education and Library Boards' Autism Services. For such support, a confirmed diagnosis of an autistic spectrum disorder (ASD) is not required.
2. Current Legislative Base
The Education (NI) Order 1996 and the Special Educational Needs and Disability (NI) Order 2005
2.1 Special Educational Needs (SEN) legislative framework
The SEN legislative framework consists of:
- primary special education legislation;
- special education regulations; and
- the Code of Practice (CoP) on the Identification and the Assessment of Special Educational Needs and the supplement to the CoP.
2.2 General
Children with autistic spectrum disorder (ASD) fall within the definitions of both 'special educational needs' and 'disability', as described in the paragraphs below. Children with ASD therefore have the same rights in education under current SEN and disability discrimination legislation as, for example, children with physical or sensory disabilities, children with severe or moderate learning difficulties and children with conditions such as attention deficit disorder (ADD), attention deficit hyperactivity disorder (ADHD) or dyslexia. These definitions are comprehensive and cover SEN and disabled children, whatever the basis for the need. The definitions are also compatible with the Section 75 duties of the NI Act 1998, in that they promote equality of opportunity between persons with a disability and persons without, and do not distinguish between any one type of disability to the detriment or exclusion of another.
2.3 The Education (NI) Order 1996
Under the Education (NI) Order 1996, the statutory responsibility for securing provision for pupils with special educational needs, including those with ASD, rests with the five ELBs and schools, which are responsible under special education legislation for identifying, assessing and, in appropriate cases, making provision for children with special educational needs in their areas/schools. The Code of Practice on the Identification and Assessment of Special Educational Needs (DE, 1998) has brought clear guidelines for all professionals working with children with SEN and one of its fundamental principles is that the individual needs of all pupils who may experience learning difficulties during their school careers must be addressed. The CoP sets out a 5-stage SEN framework for ELBs and schools to follow.
2.4 Special Educational Needs and Disability (NI) Order 2005 (SENDO)
SENDO came into effect on 1st September 2005 and strengthened the rights of all children with SEN to a mainstream education, and for the first time introduced here disability discrimination laws for the whole education sector, including institutions of further and higher education. In 2005 the Department of Education issued, for schools and ELBs, a Supplement to the existing Code of Practice on the Identification and Assessment of Special Educational Needs, in order to support the new SEN provisions of the SENDO. Additionally the Equality Commission for NI (ECNI) has issued a Disability Discrimination Code of Practice for Schools outlining their responsibilities under the disability discrimination aspects of SENDO.
2.5 Main SEN Provisions of the Education (NI) Order 1996
The main provisions of the Education Order (NI) 1996 are as follows:
- a definition of 'special educational needs': a child has special educational needs if he/she has a learning difficulty which calls for special educational provision to be made for him/her;
- a definition of 'learning difficulty': a child has a learning difficulty a) if he/she has a significantly greater difficulty in learning than the majority of children of his/her age or b) if he/she has a disability which either prevents or hinders him/her from making use of educational facilities of a kind generally provided for children of his/her age in ordinary schools or c) he/she has not attained the lower limit of compulsory school age and is, or would be if special educational provision were not made, likely to fall with a) of b) when he/she is of compulsory school age;
- a general duty on ELBs to determine, of the children for whom they are responsible, the special educational provision called for by any learning difficulty;
- a qualified duty on ELBs to secure education in ordinary schools for a child for whom the board maintains a statement of SEN;
- duties on Boards of Governors of ordinary schools to make the necessary SEN provision for registered pupils, secure that for those pupils with SENs, their needs are made known to those teaching the pupils and secure that teachers are aware of the importance of identifying and providing for those registered pupils with SEN;
- allows ELBs to request the help of a health and social services authority in order to determine a child's needs;
- requires a health and social services authority to comply with such a request, (but significantly allows the authority to have regard to the resources available to it when considering if it will comply with the request or make provision);
- duties on ELBs under the statutory assessment and statementing framework, which require that the educational provision outlined in a statement is arranged by ELBs; and
- requires DE to establish a Special Educational Needs Tribunal (now the Special Educational Needs and Disability Tribunal under SENDO) to hear appeals by parents on certain aspects of ELB assessment and provision.
2.6 Main SEN Provisions of the Special Educational Needs and Disability (NI) Order 2005 (SENDO)
The main SEN provisions of the SENDO are to:
- strengthen the rights of children with SEN to be educated in ordinary schools, where parents want this and the interests of other children can be protected;
- require ELBs to make arrangements for services to provide parents of children with SEN with advice and information (an Advice and Information Service was established in 2005);
- require ELBs to provide a means of resolving disputes between parents and schools or ELBs (a Dispute Avoidance and Resolution Service - DARS - was established in 2005);
- require the Department of Education to reform the Special Educational Needs Tribunal to become a Special Educational Needs and Disability Tribunal (SENDIST), in order to hear both appeals about SEN provision and claims about disability discrimination;
- require Boards to comply, within prescribed periods, with orders of the SENDIST and make other technical changes in support of the Tribunal process and the statementing process;
- require schools to inform parents where they are making special educational provision for their child;
- allow Boards of Governors or proprietors of schools to formally request a statutory assessment of a pupil's SEN; and
- allow parents to appeal to SENDIST where another body has requested a statutory assessment.
2.7 Main Disability Provisions of SENDO
The main disability discrimination provision of SENDO, insofar as they relate to ELBs and schools (including independent schools), are:
- a definition of disability (from the Disability Discrimination Act 1995) which states that a person has a disability if he/she has a physical or mental impairment, which has a substantial and long-term adverse effect on his/her ability to carry out normal day-to-day activities;
- a duty not to treat pupils who have a disability less favourably, without justification, for a reason which relates to their disability;
- a duty to make reasonable adjustments so that pupils who have a disability are not put at a substantial disadvantage compared to pupils who do not have a disability;
- a duty to plan and make progress in increasing accessibility to school premises and the curriculum, and in improving ways in which information is provided to pupils with a disability. The SENDO provisions prohibit schools from discriminating against disabled children in their admissions arrangements, in the education and associated services provided by the school for its pupils and in relation to its exclusions from school.
It should be noted that the duty of reasonable adjustments on schools does not require the provision of auxiliary aids and services or the removal or alteration of physical features. Decisions about the provision of educational aids and services for children continue to be taken within the SEN framework.
3. Special Educational needs and ASD: Statistics and Prevalence
3.1 Educational Statistics
Statistics in relation to all SEN pupils in schools are collected annually through the Department of Education's school census. For pupils with ASD, data is collected under the two separate headings of 'autism' and 'Asperger's syndrome'.
3.2 The School Census figures show that in 2002 there were 1,158 pupils with ASD (autism or Asperger's syndrome) reported by schools as receiving special educational provision at stages 1 to 5 of the Code of Practice. These figures rose in 2009 to 3,973[1] pupils with ASD.
The reported level of ASD in schools[2] of children, at stages 1 to 5, with ASD diagnoses or assessments, has therefore increased by 243% between 2002 and 2009.
3.3 We can compare the increase in the levels of ASD with the overall levels of children recorded in the school census as having SEN, across all types. In 2002 there were 46,285 pupils reported with SEN, including 10,339 with statements. By comparison in 2009 the school census reported 63,107 children with SEN at stages 1-5 (including pre-school), including 13,574 with statements. This represents an overall increase between 2002 and 2009 of 36.3% in the incidence of pupils with a SEN at stages 1-5. The growth in the prevalence of the numbers of pupils with ASD, has, therefore, increased at a significantly greater rate than the increase in overall numbers of SEN pupils across all areas.
3.4 In addition, we can compare the numbers of children with ASD with those with other types of SEN. The table below set out the numbers of children in the 10 most prevalent SEN categories, as recorded in the school census in 2009. ASD/Asperger's Syndrome is ranked 7th in relation to other SENs, with over 4,000 pupils recorded on the spectrum.
Prevalence of SEN* 2009/10 across Pre-Schools, Nursery Schools, Primary Schools, Post Primary Schools & Special Schools (Stages 1-5)
| Ranking | SEN | Number |
| 1 | Mild Learning Difficulties | 15,304 |
| 2 | Cognitive & Learning (general) | 10,044 |
| 3 | Speech & Language | 8,650 |
| 4 | Moderate Learning Difficulties | 8,265 |
| 5 | Dyslexia | 6,568 |
| 6 | SEBD | 6,316 |
| 7 | Autism/Asperger's | 4,004 |
| 8 | ADD/ADHD | 2,353 |
| 9 | Other | 2,099 |
| 10 | Severe Learning Difficulties | 2,049 |
*All SEN needs
4. Educational Resources for ASD
4.1 The entire area of SEN resources, and in particular those for ASD, has been a priority for DE since the Report of the Task Group on Autism was launched in 2002. The bulk of SEN resources are allocated via the ELBs' block grant, although considerable funding has been earmarked, by DE, in order to meet specific pressures. ELBs determine annually, according to their priorities, how the allocation of the block grant is made.
4.2 In 2009/10 around £172m was expended by ELBs from the block grant for provision for children with special educational needs. Since the publication of the Task Group Report on Autism, DE has secured additional resources totalling some £9.3m to support positive measures in ASD. These include:
- ASD-related training within the pre-school sector, to teachers, classroom assistants, playgroup leaders and assistants, qualified early years specialists and relevant ELB staff;
- funding to ELBs to enable key staff to undertake accredited training in Applied Behavioural Analysis;
- the formation, in 2003/04, of the Inter-board ASD Group to promote commonality and consistency of approach in relation to identification, assessment and delivery of services to children with ASD across the five ELBs and develop cross-Board training for ELB staff and schools in a range of ASD strategies and interventions;
- the production of a range of school/parent resources to support positive interventions for children with ASD, issued to all schools, ELBs and ASD voluntary groups, as aids to teachers and classroom assistants and to provide information to parents. These include: complementary parent and teacher videos/ DVDs/CD-ROMs and guidance material on ASD, produced by DE on a North/South basis; "ASD a Guide to Classroom Practice"; "Evaluating Provision for Autism"; and "Opening the Spectrum", a resource pack produced on a cross-border basis.
5. Task Group Report on Autism
5.1 The Report of the Task Group on Autism in May 2002, which was a major milestone in understanding the educational needs of young people on the autism spectrum, provided DE with an agenda for a 10-year period to address its recommendations. The Task Group found that within the previous few years educational, health and social services provision for children and young people with ASD had entered a period of rapid improvement in many areas. However, that there was still much progress to be made before it would be possible to say that all children and young people with ASD were being identified and that their needs were being fully met. The Group reported that there was, in particular, a demand for more prompt access to diagnostic services at an early age and that these services should be followed immediately by effective interventions. Considerable concern was expressed in the report about provision for children with ASD and challenging behaviour.
5.2 The report contained a range of recommendations and stressed the need for significant improvements in 3 main areas:
- access to multi-agency, multi-disciplinary diagnostic and assessment services;
- training for parents of, and people who work with, children and young people with ASD; and
- school-based and home-based educational and therapeutic provision
5.3 As a consequence of the report, DE made a commitment to provide schools and parents with improved educational services and support. The actions undertaken since contribute to fulfilling the commitment to raising the standards and improving the provision for this group of young people, with significant additional funding to support the recommendations contained in the Task Force report. Key measures and actions which have been implemented since the publication of the report are listed in paragraph 3.3 above.
6. The Education and Training Inspectorate (ETI) Report – An Evaluation of the Inter-Board Autistic Spectrum Disorder Advisory Service
6.1 The ETI survey report in October 2008: "An Evaluation of the Inter-Board Autistic spectrum Disorder Advisory Service" provided definitive evidence of the good, very good and sometimes excellent work of the ASD advisory teams across the boards. The team of inspectors visited some 67 schools, interviewed principals, teachers, autism advisors and the senior managers of the inter-board service. In addition, a small number of parents and pupils were interviewed.
6.2 The survey suggested the following key improvements would help to deploy the excellent collective knowledge and expertise of the autism teams:
(i) the re-structuring of the five board services into a single Regional Autistic Spectrum Advisory Support Service;
(ii) the development of a more robust and rigorous pre-school support programme in tandem with the department of Health and Social Services and Personal Safety; and
(iii) the development by DE of a strategic policy for autism, to inform the educational planning and service delivery with the key stakeholders, including other relevant government departments.
6.3 The survey concluded by commenting:
"The DE initiative is to be commended for its response to the 2002 Autism Report and the development further by the boards of their autism advisory services celebrated on the practical achievements to date and the capacity to improve further. Addressing the inconsistencies in provision and the gaps in pre-school provision are key to this development. It is now time to develop a regional advisory service for autism and an autism strategic plan for Northern Ireland. The autism advisory services have demonstrated the capacity to support this process."
7. DE Autism Strategy and Implementation Plan
7.1 In light of a range of developments, additional funding and the recommendations contained in the ETI report: "An Evaluation of the Inter-Board Autistic spectrum Disorder Advisory Service", the Minister for Education agreed, in October 2009, to commence a review of the Department's ASD policy and to develop an education sector autism strategy and implementation plan for children and young people on the autism spectrum to ensure further and future development in this area.
7.2 As part of the development of the strategy a mapping exercise was undertaken during 2010, in collaboration with our education and health partners and international experts in the field of autism. The mapping exercise has been undertaken within the context of the 2002 Task Group Report on Autism, the 2008 ETI evaluation of the Inter-Board ASD Advisory service, recent research, prevalence trends and the many examples of good, innovative practice that have developed since the publication of the 2002 Task Group Report. Pre-consultation with voluntary groups, higher education institutions, parents, trade unions, the Middletown Centre for Autism and the Regional Strategy Group for Special Education commenced in October 2010.
This work has been developed in conjunction with the work undertaken by the Department of Health, Social Services and Public Safety which has already introduced a framework for the development of health related services for young people with autism and their families.
7.3 The mapping exercise has identified several strategic areas for development in conjunction with education and health partners.
Key areas include:
- collaboration between DE and DHSSPS to ensure continuity in policy and strategic approaches;
- further collaboration between ELBs and Health Trusts to promote uniformity and cohesion in health and education provision;
- addressing the increasing demand on resources to ensure more equitable and effective provision; and
- shaping policy development through local and internationally based research.
7.4 An autism strategic framework and implementation plan for the education sector will be developed which will establish a direction for the further development of educational services and provision for children young people on the autistic spectrum. The strategic framework and implementation plan will aim to enhance the educational outcomes for children and young people on the autistic spectrum and across the ability range up to the age of 19. This will be achieved through the provision of a continuum of educational services and provision, taking cognizance of the actions and plans of other agencies which impact on or complement education.
[1] Includes pupils attending nursery, primary, post-primary and special school settings. Data relating to SEN type was not available for pre-schools in 2002. In 2009, 31 children with ASD were recorded in pre-school settings, giving an overall total of 4,004 children recorded across all school settings.
[2] Excluding pre-school settings
Department of Health, Social Services and
Public Safety
Introduction
1. The purpose of this paper is to update members of the Health and Social Care Committee on the Departmental view on the Private Member's Autism Bill, in advance of the oral evidence session scheduled for 20 January 2011. The key points remain those outlined in our paper of 29 November 2010 and covered in the oral evidence presented to the Committee on 2 December. For ease of reference, the previous Health Committee submission (Appendix A) is appended.
2. The Department has significant concerns regarding the content and quality of the Bill and remains of the view that legislation is not required to drive forward service improvement; the focus should be on the application of all available resources to the enhancement of front line services rather than on legislation and the bureaucracy which will inevitably come with it.
3. This paper concentrates on issues relating to:-
- Amendments to DDA;
- Competence of the Bill, and clarity of intent;
- Cost; and
- Bureaucracy arising from the Bill.
Amendment to DDA
4. Clause 1 of the Bill includes amendments to the Disability Discrimination Act 1995 to include the words – "social (including communication)" and amendment to Schedule 1 to include "taking part in normal social relationships" and "forming social relationships".
5. You will be aware that responsibility for anti-discrimination legislation, including for those with disabilities, rests with OFMDFM. In such circumstances, the Committee might wish to seek the advice of the relevant department regarding any proposed changes to the DDA.
6. It remains this Department's view, as stated previously, that autism is already embraced by the DDA, as evidenced in practice by case law. In addition, the proposed non specific changes could have far reaching negative effects on individuals and society which may not have been intended by the proposer of the Bill.
7. It is also of note that proposed changes to the DDA, in our view, will not have the desired effect of increasing access to Social Security Benefits (as suggested); for example, Disability Living Allowance is based on the impact/disability arising from a condition and not the condition itself.
8. However, legislation and regulations on access to social security benefits fall within the remit of the Department of Social Development (DSD). Any further detailed information should be sought from that Department.
Competence and Clarity of Intent of the Bill
9. Clauses 2 and 3 provide for the formation and content of the autism strategy. From a policy perspective, it remains uncertain what the proposed strategy (as outlined in the Bill) is designed to do. This is especially so as there is already in place an ASD strategic action plan and an infrastructure to deliver it.
10. The Bill is stated as having no significant cost, yet it might be argued that the Bill's intent is to improve the rights of individuals and their carers to have needs met. This could not be achieved without significant cost. Hence, the intention is not clear. It should be noted that the approach taken in this Bill is somewhat different to that of the Autism Act 2009 which clearly defines duties and responsibilities within the Autism Strategy.
11. In addition, Health Committee members will be aware that, in December 2010, the Committee for Education, Lifelong Learning and Culture in Scotland (the Committee to which the lead on the Autism (Scotland) Bill was allocated) rejected the Bill - expressing concern that the bill may not deliver the required improvements. It stated:-
"… the committee is not convinced the proposed Scottish Government strategy on autism would be improved by passing of autism specific legislation"
" we are also concerned this bill could create a perception of two- tier disabilities, with some strategies thought of as more worthy of legislation and therefore seen as having more weight.
12. The Bill was debated at Stage 1 in the Scottish Parliament on Wednesday 12 January 2011 and was rejected by 109 votes to 5 with 2 abstentions.
13. In respect of the Autism Bill (NI), the Department has no policy rationale to underpin the development of this piece of legislation. Indeed, some concern has been expressed that such a Bill might possibly be subject to challenge under the European Convention on Human Rights, particularly in relation to individuals and families living with other significant disabling conditions.
14. Given the above paragraphs, the Health Committee may wish to consider the legislative competence of the Assembly in relation to the provisions of this Bill.
Cost
15. Unlike the Autism Bill in England, this Bill indicates that there is little cost attached. In Scotland, a Financial Memorandum was attached to the autism legislation, and included costings but chose not to include costs for the implementation of the Bill.
16. It is difficult to understand how 'no significant costs' have been assessed. For example, the inclusion of such non-specific terminology within the amendment to the DDA such as "social (including communication)" and "taking part in social normal social relationships and forming social relationships" may bring individuals (without autism) within the scope of the Disability Discrimination Act. Such an approach could have significant human cost for individuals and families and could have significant financial costs for organisations that would be required to take account of such non-specific "disabilities".
17. In addition, each government department would need to make an assessment of the impact of the change to the Disability Discrimination Act, and the placement of the definition of autism (Clause 4) on the face of the legislation.
Cost of the strategy
18. The cost of formulation of a rolling and indefinite autism strategy is not specified nor is the need to establish extensive monitoring arrangements. This could be extensive.
Cost of Training
19. In addition, whilst no costings have been done by the Bill sponsors for the required public awareness raising or training of front line civil servants the Department has attempted to develop indicative costs for both requirements. Training for civil servants brings a potential cost of some £1.8m (based on circa 25,500 civil servants at £65 per head).
20. Whilst that is the requirement of the legislation we would contend that such training would not actually encompass the key target staff i.e those in the public sector employed in providing front line services in education, health and social care, hosing and many other areas.
Awareness
21. It is difficult to calculate the potential cost of public awareness-raising without some parameters to define the extent of the campaign. However, advice from the Government Advertising Unit suggests that awareness campaigns are largely designed to fit the allocated budget. For example a budget of £25k will provide a small advertising campaign (largely using existing print and radio material); £235k can provide development of new material for all media, limited TV, press online and radio adverts, modest outdoor advertising e.g. on buses and bus shelters and some benchmarking and tracking research.
Increased Bureaucracy arising from Autism Bill
22. Through the current Regional ASD Network Group, work has been undertaken with minimal bureaucracy and without the need for legislation. This highlights the commitment of the DHSSPS to enhance ASD provision.
23. The Department continues to have concerns that the introduction of specific autism legislation, at this time, could be disruptive to the ongoing work of the Regional Group, could delay the implementation of the current ASD Strategic Action Plan, and would create a bureaucratic and costly approach to the development and monitoring of a new ASD Strategy.
24. The following paragraphs highlight the work of the Regional ASD Network Group which leads on the implementation of the DHSSPS ASD Strategic Action Plan 2009.
25. The ASD Strategic Action Plan is underpinned by an additional £1.5 m specifically for autism services. This will rise to £1.6 million (recurrent) from April 2011 following the Minister's announcement in November 2010 of an additional £100k towards developing specialist adult autism diagnostic services.
26. Significant improvements in autism services, led by the Network Group, include the reduction in waiting times for ASD assessment and diagnosis in children, despite increasing demand.
27. In addition, in November 2010, the Minister announced the development of a regional Diagnostic Pathway for Children and Young People for implementation from December 2010 and the development and commencement in 2011 of a diagnostic service for adults with autism.
Conclusion
28. The DHSSPS does not need an Autism Bill to facilitate change. It wants to assure the Committee of its intention to continue to improve autism services for both children and adults, within the resources available to it.
29. The potential costs arising from the Bill are substantial. It will bring significant additional costs in bureaucracy, infrastructure, poorly targeted training and impose an onerous requirement on this Department to monitor and report performance across other Departments.
30. The DHSSPS does not wish to spend resources on bureaucracy but rather concentrate on agreed priorities, which are directed towards frontline services.
31. The impact of this Bill has also the potential to be significant for other Departments' policies and legislation. The Committee will wish to consider whether specific advice on issues relevant to other Departments should be secured.
32. Having taken legal advice, it is the Department's view that there are potential significant and far reaching implications arising from this Bill, with particular reference to Clauses 1, 2 and 3. The Committee will wish to consider the impact of ECHR and whether Clauses 2 and 3 might call in to question the legislative competence of the Assembly in relation to the provisions of this Bill.
January 2011 - DHSSPS
Appendix A
Autism Bill (Private Member's) - DHSSPS Perspective
(Submitted to Committee in November 2010)
Introduction
1. The purpose of this paper is to provide an up to date Departmental view on the detail of the Private Member's Autism Bill which was introduced in the Assembly on 8 November 2010. In doing so, it is recognised that an Executive view of the Bill is being sought by Minister McGimpsey to inform the debate on the second stage of the Bill which is scheduled for the 7 December 2010. Therefore, this paper confines itself to the impact of the Bill on DHSSPS policy responsibilities.
Background
2. This Autism Bill is a Private Member's Bill which has been developed by the All Party Group on Autism supported by Autism NI which provides the secretariat to this Group. The Department's view on the need for legislation on autism has already been submitted to the Committee on 28 September 2009.
3. Whilst recognising that the content of the proposed Bill has changed since it was last discussed with the Health Committee on 1 October 2009, the Department remains of the view that legislation is not required, at this time, to drive forward service improvement; the focus should be on enhancement of front line services not on legislation. This view is complemented by the Independent Review of Autism Services (2008), which did not support legislation but highlighted the need for significant service developments to meet the needs of those living with autism. As a consequence, the DHSSPS published an ASD Strategic Action Plan in 2009. As part of this Plan, a Regional ASD Network Group was established and is now operational and includes involvement of 30 parents, service users and carers, together with 10 key voluntary organisations in decision-making.
4. The ASD Strategic Action Plan is underpinned by an additional £1.5 m specifically for autism serivces. This will rise to £1.6 million (recurrent) from April 2011. The Regional Network, with significant involvement from the Reference Group, is responsible for the coordination of the regional approach to service development and investment.
5. Significant improvements in autism services include the reduction in waiting times for ASD assessment and diagnosis in children despite increasing demand, the development of a regional Diagnostic Pathway for Children and Young People for implementation from December 2010 and the development and commencement in 2011 of a diagnostic service for adults with autism. All of this work has been undertaken without the need for legislation and highlights the commitment of the DHSSPS to ASD provision.
Detail of the Autism Bill
6. The Department has significant concerns that the introduction of an Autism Bill, at this time, could be disruptive to the ongoing work of the Regional Group, could delay the implementation of the current ASD Strategic Action Plan, and would create a bureaucratic and costly approach to the development and monitoring of a new ASD Strategy.
7. More specifically, the Department has significant concerns regarding:-
- the unilateral change in definition to the Disability Discrimination Act, which has not been done in other UK jurisdictions;
- the insertion of a wide definition of autism in legislation, which has not been done in other jurisdictions of the UK (and its impact on individuals and society);
- Cost – it is stated that the Bill will not have significant cost implications – the Department disagrees with this statement;
- Autism Strategy – the necessity for legislation to do this is not proven – particularly when infrastructure is already in place.
- Data collection – legislation is not needed to collect prevalence data (see also below).
Amendment to Disability Discrimination Act 1995 (DDA)
8. The Bill includes amendments to the Disability Discrimination Act 1995 to include the words – "social (including communication)" and amendment to Schedule 1 to include "taking part in normal social relationships" and "forming social relationships";
9. The changes to the DDA are significant, as the inclusion of wording such as "social (including communication)" as a disability could be open to wide interpretation and might have the potential for challenges to be taken by others in society/workplace that do not have autism. In addition, it should be noted that in England, the Autism Act 2009 does not have such amendments to the DDA. Nor does the recently proposed Autism Bill in Scotland. Given that existing case law appears favourable to the inclusion of the symptoms of autistic spectrum disorders, the Department cannot see the benefit of the proposed new definition – further, the proposal may actually be harmful if it were to cast doubt on the DDA definition as it would continue to apply in GB, as the DDA is a Westminster enacted, UK wide act, and the Assembly has no power to amend it as it applies to England, Scotland and Wales. It should also be noted that guidance issued here from OFMDFM – Guidance on matters to be taken into account in determining questions relating to the definition of disability - already recognises that that a disability can give rise to a wide range of impairments which may not be immediately obvious. A number of specific examples are given in this document including autistic spectrum disorders.
Inclusion of Definition of Autism in the Legislation
10. The Bill also introduces a wide definition of autism to include several established syndromes in addition to adding "any pervasive developmental disorder not otherwise specified" - all within the definition of "autism". Such a definition is outside of the meaning of autism as used in standard clinical practice guidance - as defined within the International Classification of Diseases (ICD 10). Within this context, there is an established definition of pervasive development disorder. It includes childhood autism, atypical autism, Asperger's Syndrome, but also other coded categories. It should be noted that the recent proposed Scottish legislation does not include a definition of Autism on the face of the legislation - it explains that to do this is not advantageous "as research and experience refines the understanding of autism, so the range and characteristics will change. It is because of this that no definition of the autistic spectrum condition has been included".
11. Clearly a unilateral approach to the definition of autism to be included on the face of NI legislation is not advantageous and could adversely impact on the labeling of individuals. In addition, this also has the potential to adversely impact on data collection on the prevalence of "autism".
12. The objective of current health and social care services is to provide appropriate care and support based on individual patient needs rather than a specific diagnostic label. This allows greater efficiency in delivering services within a programme of care rather than dividing efforts according to diagnosis. Trusts also have the appropriate level of flexibility to meet priorities, particularly important with a condition covering a spectrum of abilities.
Cost
13. Unlike the Autism Bill in England, this Bill has no finance clause; hence, it erroneously implies that this Bill has little cost attached. In Scotland, a Financial Memorandum was attached to the autism legislation, and included costings but chose not to include costs for the implementation of the Bill.
14. The NI Autism Bill is more extensive than either England (which is adults only) or Scotland which primarily relates to development of an autism strategy. As no financial memorandum has been attached to the NI Bill, it is difficult to understand how no significant costs have been assessed. For example, the inclusion of such non-specific terminology within the amendment to the DDA such as "social (including communication)" and "taking part in social normal social relationships and forming social relationships" may bring individuals (without autism) within the scope of the Disability Discrimination Act. Such an approach could have significant human cost for individuals and families and could have significant financial costs for organisations that would be required to take account of such non-specific "disabilities".
15. The cost of formulation of a rolling and indefinite autism strategy is not specified nor is the need to establish extensive monitoring arrangements. In addition, no costs have been attributed to public awareness raising, or training of front line civil servants. It also gives a mandate to DHSSPS for this strategy and its monitoring, without necessarily having the power to facilitate change outside of a health and social care environment.
Autism strategy
16. Legislation is not needed to effect service change or to develop an autism strategy – DHSSPS consulted upon and issued a Strategic Action Plan in June 2009, and DE is well advanced in producing a detailed autism strategy which will be published for consultation in
17. 2011. The Regional ASD Network Group, which is part of the DHSSPS Action Plan, is already in place and provides an annual written report on its actions. It has considerable voluntary sector, parental and service user involvement through its Reference Group. Good progress is being made to enhance service provision especially to reduce waiting times for diagnostic assessment and to develop a diagnostic pathway for children and young people. This regional Diagnostic Pathway has been agreed for implementation from December 2010. In addition, further investment has been secured in November 2010 to commence development of adult diagnostic assessment and treatment services in each Trust in 2011.
18. Through the Regional Network, the Department's focus has been to involve parents, carers and the voluntary sector organizations in commissioning and development of autism services. In doing this, there is a focus on reduction of administration and diverting all available resources towards improving and creating front line services. This Bill, if enacted, does not sit well with this policy as further resources will have to be diverted towards development of a strategy, thus cutting across existing strategies. In addition, the Bill implies a cost neutral environment for all government departments; clearly this could not be the case and even the production of a cross departmental equality impact assessment and monitoring arrangements for the strategy would require investment. In addition, an autism public awareness campaign and steps to train NI Civil Service staff in direct contact with the public would require investment.
Prevalence Data
19. It is recognised that data collection is important and that more information is needed in regard to the prevalence of autism (children and adults). Legislation is not needed to improve prevalence data. As part of the ASD Strategic Action Plan, HSC Trusts are currently working on improvements to their data collection on ASD as part of their service improvements and it is anticipated that this will be quality assured across Education Databases to ensure consistency.
Conflict with existing legislation
20. As noted above, unilateral changes to the DDA may cause some difficulties on a UK wide basis. In addition, Members will wish to note that Section 75 of the Northern Ireland Act 1998 does not apply to this Bill since it is a private member's Bill and is not being introduced by a public authority. The sponsor is, therefore, not required to carry out an Equality Impact Assessment on the Bill. However, any autism strategy, developed by the DHSSPS, with the involvement of other Government Departments would be subject to Section 75 of the NI Act.
21. Each government department would need to make an assessment of the impact of the unilateral change to the Disability Discrimination Act, and the definition of autism – given their broad nature.
Conclusion
22. Good progress is already being made to enhance service provision for those living with autism. No legislation is required to produce an autism strategy; indeed the introduction of an indefinite autism strategy underpinned by legislation may have the potential to do harm as it could dismantle the progress that has been made to date.
23. The focus should be on improvement of frontline services for those living with autism rather than the diversion of resources to the proposals in this Bill. Therefore, on the basis of current autism policy developments, cost and potential significant implications for the Disability Discrimination Act, and the potential negative impact of putting a circumscribed definition of autism in legislation, this Bill is not supported by the DHSSPS.
24. No comment is made on the legislative competence of this Private Member's Bill. This is a matter for the member.
Department of the Environment
Office of the First Minister and deputy First Minister
Department of Justice
Appendix 4
Other Evidence
30 November 2010
Autism Bill
NIAR 591-10
This Paper provides information to support consideration of the Autism Bill, which was introduced into the Assembly on 8th November 2010. The Autism Bill aims to enhance the provision of services to and support for people with conditions which are on the autistic spectrum. The Bill sets out to achieve this by:
(1) amending the Disability Discrimination Act 1995 so as to resolve any ambiguity as to whether the term disability applies to autistic spectrum conditions; and
(2) requiring the preparation and implementation of an autism strategy
Paper 181/10 30 November 2010
Research and Library Service briefings are compiled for the benefit of MLA's and their support staff. Authors are available to discuss the contents of these papers with Members and their staff but cannot advise members of the general public. We do, however, welcome written evidence that relate to our papers and these should be sent to the Research & Library Service, Northern Ireland Assembly, Room 139, Parliament Buildings, Belfast BT4 3XX or e-mailed to RLS@niassembly.gov.uk
Executive Summary
The Autism Bill, which was introduced into the Assembly on 8th November 2010, aims to enhance the provision of services to and support for people with conditions which are on the autistic spectrum. The Bill sets out to achieve this by:
(1) amending the Disability Discrimination Act 1995 so as to resolve any ambiguity as to whether the term" disability" applies to autistic spectrum conditions; and
(2) requiring the preparation and implementation of an autism strategy.[1]
Section 2 of this paper provides information relating to the Bill's amendments to the Disability Discrimination Act (DDA), which in Northern Ireland is the primary piece of legislation which protects those with a disability from discrimination. In spite of guidance and case law which indicate that, in a range of circumstances, the DDA can be relied upon by those with autistic spectrum conditions, there is continued ambiguity as to whether autistic spectrum conditions fall within the definition of disability contained within the DDA. The Bill provides for amendment of the DDA in two ways in an attempt to resolve this ambiguity.
The DDA currently refers to mental and physical impairments and the Bill adds a third category of impairment, namely, 'social (including communication) in an attempt to broaden the scope of the definition of disabled person in a way which more clearly encompasses those with autistic spectrum conditions. This widenening of the definition should mean the DDA would also more easily encompass other behavioural disorders, such as 'Anxious [avoidant] personality disorder'.
In a further attempt to make access to the protections of the DDA more accessible to those with autistic spectrum conditions, the Bill provides for additions to the list of day-to-day activities set out in the DDA. A person's impairment must have a substantial and long-term adverse effect on their abilitity to carry out normal day-to-day activities for them to have a disability for the purposes of the DDA. The Bill adds the following two 'day-to-day' activities to those already contained in the DDA:
taking part in normal interaction or
forming social relationships.
The DDA has been repealed in England, Scotland and Wales and the Equality Act 2010 is now the primary piece of legislation which protects those with a disability from discrimination in a range of areas. The Equality Act defines disability in a similar way to the DDA but, whilst making reference to day-to-day activities, does not define those within the Act. The Equality Act makes reference only to physical and mental impairments. The Office for Disability Issues, the body set up to co-ordinate disability policies across the UK Government, however, has published a consultation document on guidance for defining disability within the context of the Equality Act.
In the Republic of Ireland, the Disability Act 2005 uses a definition of disability[2] which refers not only to physical and mental health impairments but also to sensory and intellectual impairments. There is no reference, however, to social or behavioural impairments. Whilst the definition in the Disability Act 2005 refers to participation in social life, the legislation provides no further information as to what this refers.
Section 3 of this paper focuses on the provisions within Clause 2 of the Bill and how these compare with relevant provisions in the Autism Act 2009 and the Autism (Scotland) Bill, which both require the production of autism strategies. There is no legislative requirement on government to produce an autism strategy in Wales or the Republic of Ireland.
Clause 2(1) of the Bill places a duty on the Department of Health, Social Services and Public Safety (DHSSPS) to prepare and publish a strategy on autism within two years of the bill becoming an Act. DHSSPS must consult with the Northern Ireland departments before preparing the autism strategy and must request that every HSC trust provide data on the prevalence of autism in its area in order that the strategy can be published, implemented and updated (Clauses 2 (3)-(4)).
Clause 2(5) places a duty on the DHSSPS to review the strategy and publish a revised strategy at intervals of not more than seven years. The Department is required to monitor the implementation of the strategy by all the Departments (Clause 2(6) and all the Departments must co-operate with the DHSSPS as regards preparation, review and implementation of the strategy with regard to the parts that fall within their areas of responsibility (Clause 2(7), (8)). Clause 2(9) provides for the publication of an implementation report by the DHSSPS on the strategy every three years from publication.
Section 4 of the paper briefly outlines the existing strategies and action plans in Northern Ireland, England and Wales. It also outlines the content of the draft strategy that has recently been published in Scotland. In the Republic of Ireland, a National Review of Autism Services is currently being undertaken by the Health Service Executive and it is expected that a final report will be presented to the Health Service Executive Board later in 2010 or early in 2011.
In Northern Ireland, the DHSSPS published an Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11 (June 2009). Whilst the Action Plan is primarily focused towards health and social care services, it notes the importance of partnership working to promote a person-centred approach to ASD service provision. With regard to the ASD Strategic Action Plan for Wales, published in 2008, the aim has been to take a holistic view encompassing the services offered by and across government and the voluntary sector and to include education, health, financial and social needs.[3] Wales has been heralded as the 'first European nation to commit to a 'whole nation' model for delivering high-quality services and research' into ASD.[4]
The Strategy for Adults with Autism in England (March 2010), draws on the findings of the National Audit Office report Supporting people with autism through adulthood[5] The strategy is designed to build on the progress already made in England in improving services for children with autism[6] but, in line with the requirement of the Autism Act 2010, focuses on adults only.
The Scottish Government recently published its draft autism strategy, Towards an Autism Strategy for Scotland (September 2010), which sets out what the Scottish Government in partnership with users, carers and professionals proposes to do to meet the needs of people with ASD. The Autism Spectrum Disorder Reference Group that led earlier work in Scotland from 2002 and 2008 has been reconvened and will be expanded to provide leadership for the strategy.
Clause 3 of the Bill sets out in further detail the proposed content of the autism strategy and Section 5 of this paper reviews this clause in the context of the existing strategies and action plans outlined above.
Clause 3(1) states that the strategy 'must set out how the needs of persons with autism are to be addressed throughout their lives'. In a lifelong approach, the points of transition in an individual's life are prioritised in all the strategies and action plans. It appears that it is in the area of transitions that the cross-cutting nature of services and co-operation between government departments, agencies, voluntary and community groups etc. becomes most important.
Clause 3(2) prescribes that the autism strategy shall include the health care, educational and social needs of persons with autism. The current DHSSPS Action Plan focuses primarily on health and social care services for those with ASD with five key themes linked to the central tenet of the Care Pathway for ASD.
The overall direction for health and social care service redesign in the Action Plan for Wales is based on its approach for developing all health and social services based on the concept of a four level/four tier strategic conception of their functions. Some of the main areas the Welsh strategy focuses on are: mapping prevalence; needs and services; supporting the establishment of a multi-agency ASD co-ordinating group in each local area; quality Standards in Education for Pupils with ASD; and clear arrangements for transitions including key transition workers to support to children and young people with SEN (including those with ASD) as they move through school to further education or the workplace.
Within the current English strategy for adults with ASD, two of the five core areas of focus are relevant to health and social care needs: the development of a clear, consistent pathway for diagnosis in every area, which is followed by the offer of a personalised needs assessment; and improving access to the support needed to live independently. Of the remaining core areas, two focus on the wider spectrum of needs including helping adults with autism into work and enabling local partners to plan and develop services for adults with autism to meet identified needs.
The draft strategy for Scotland focuses on outlining what still needs to be done in Scotland to build on the work already achieved by the ASD Reference Group and lists twenty six specific recommendations for action, many of which cover the areas of health, education and social needs people with autism.
Clause 3(3) of the Bill prescribes that the strategy for Northern Ireland must set out how the needs of families and carers for persons with autism are to be addressed. Within the current DHSSPS Action Plan, the principles of family support services for will be informed by the strategic context set out in Families Matter: Supporting Families in Northern Ireland (March 2009). A key action is the production of a communication plan to provide information to people with ASD, their families and carers
The Family and Carer support services section of the Welsh Strategy focuses specifically on the role that families and carers play in caring for (including a therapeutic input), advocating for and supporting people with ASD. Within the English Strategy for adults, providing relevant information to adults with autism and their families at the point of diagnosis has been identified as a key matter with statutory guidance to provide the detail of the type of information required. The current draft strategy for Scotland sees individuals, families and carers as co-producers of planning and decision-making about the best use of funding for ASD services and highlights the success to date of its Local Area Coordination and ASD Co-ordinator/Lead Officer posts .
Clauses 3(4) and (5) prescribe that the autism strategy for Northern Ireland must set out proposals for promoting an autism awareness campaign and the steps the DHSSPS proposes to take to ensure that all Northern Ireland Civil Service staff who deal directly with the public are given autism awareness training. It is worth noting that Clause 3(5) as written does not appear to cover the public servants who deal directly with the public in relation to ASD who are not Civil Servants, for example, teachers and health and social care professionals. Training and raising awareness with both professionals, patients and their families and the wider community is one of the themes of all the current action plans and strategies with various options considered, including more specialist training for front-line posts to wider awareness training.
The Explanatory and Financial Memorandum which accompanies the Autism Bill states that the bill will not have significant financial implications. However, the implementation of any strategy is where the main financial implications lie. In a press statement made on 29th November 2010, Health Minister, Michael McGimpsey announced funding of £100k to improve autism services in Northern Ireland. At the same time, he announced that it was and remained his view that '...I have all the legislative authority I need to make the necessary improvements to services...Unlike other parts of the UK the structure here gives me control over social care as well as health care'.[7]
Contents
Executive Summary
1. Introduction
2. Clause 1- Amendment to the Disability Discrimination Act 1995
3. Clause 2 - Autism Strategy
4. Existing Strategies and Action Plans
5. Clause 3 – Content of the Autism Strategy
6. Financial Effects of the Bill
1. Introduction
The Autism Bill, which was introduced into the Assembly on 8th November 2010, aims to enhance the provision of services to and support for people with conditions which are on the autistic spectrum. The Bill sets out to achieve this by:
(1) amending the Disability Discrimination Act 1995 so as to resolve any ambiguity as to whether the term" disability" applies to autistic spectrum conditions; and
(2) requiring the preparation and implementation of an autism strategy.[8]
The Bill was introduced as a Private Members' Bill by Mr Dominic Bradley, who Chairs the All-Party Assembly Group on Autism.
At present, within the UK and Republic of Ireland, the Autism Act 2009 which applies to England only, is the only existing piece of legislation directed only at autism. In Scotland, a private members bill, the content of which mirrors the content of the Autism Act 2009, was introduced to the Scottish Parliament on 26 May 2010. A table comparing the content of the Bill, the Autism Act 2009 and the Autism (Scotland) Bill is contained in Appendix 1 to this paper.
2. Clause 1- Amendment to the Disability Discrimination Act 1995
In Northern Ireland, the Disability Discrimination Act 1995[9] (the DDA), as amended, is the primary piece of legislation which protects those with a disability from discrimination. The Bill provides for amendment of the DDA in an attempt to resolve the ambiguity as to whether autistic spectrum conditions fall within the definition of the term 'disability' contained within the DDA[10]. To appreciate the nature of the ambiguity, it is necessary to consider how the DDA defines disability and how autistic spectrum conditions are defined.
DDA Definition of Disability
The DDA prohibits discrimination against 'disabled persons' in a range of circumstances, including in employment and occupation, transport, and the provision of goods, facilities and services. Only 'disabled persons', as defined in Section 1 of the DDA and associated schedules and regulations, are entitled to the protection that the DDA provides. Section 1of the DDA states the following:
Meaning of "disability" and "disabled person".
(1) Subject to the provisions of Schedule 1, a person has a disability for the purposes of this Act if he has a physical or mental impairment which has a substantial and long-term adverse effect on his ability to carry out normal day-to-day activities.
(2 ) In this Act "disabled person" means a person who has a disability.[11]
The DDA definition of who can be considered to have a disability, therefore, contains four key elements, each of which are considered in the table below.
Impairment:The definition covers physical and mental impairments. These include:
Substantial:For an effect to be substantial, it must be more than minor. The following are examples that are likely to be considered substantial:
Long-Term:Schedule 1, para 2 provides that the effect of an impairment is only a long-term effect if- (a) it has lasted at least 12 months; (b) the period for which it lasts is likely to be at least 12 months; or (c) it is likely to last for the rest of the life of the person affected. Long-term effects include those, which are likely to recur. For example, an effect will be considered to be long-term if it is likely both to recur, and to do so at least once beyond the 12-month period following the first occurrence. Day to Day activities:Schedule 1, para 4 provides that an impairment is to be taken to affect the ability of the person concerned to carry out normal day-to-day activities only if it affects one of the following:
|
Under Section 3 of the DDA, the Office of the First Minister and deputy First Minister (OFMDFM) has the power to issue guidance on matters to be taken into account in determining whether a person is a disabled person for the purposes of that Act. The guidance does not impose any legal obligations in itself, nor is it an authoritative statement of the law. However, Section 3(3) of the DDA requires that an adjudicating body (such as a court or tribunal) which is determining whether a person is a disabled person for the purposes of the DDA, must take into account any aspect of the guidance which appears to it to be relevant. The guidance issued by OFMDFM includes examples of a child with autism (p.41) and a man with Asperger's Syndrome (p.60)[12].
It has been argued that whilst Section 1, Schedule 1, and associated guidance to the DDA '...all lend support to the argument that those with an Autistic Spectrum Disorder would ordinarily fall within the provisions of the Act', the case of Hewett v Motorola[13] '...put matters beyond doubt'.[14] This case, taken in England, involved an individual whose Asperger's Syndrome was not considered by an employment tribunal to fall within the definition of disability in the DDA. The individual appealed, however, and the appeal tribunal concluded the following:
We have not found this an easy case to determine as to whether this experienced Chairman and Tribunal fell into error in their approach, but after considerable consideration, we are unanimously of the view that their approach to the concept of "understanding" was at fault in failing to acknowledge that someone who has difficulty in understanding normal social interaction among people, and/or the subtleties of human non factual communication can be regarded as having their understanding affected and that concept is not limited simply to an ability to understand information knowledge or instructions.
This case, while highlighting significant difficulties in defining the effects of ASD in terms set out in the DDA , demonstrated that features such as 'understanding' and 'social interaction' could be considered under the existing provisions of the DDA.
Definitions of Autistic Spectrum Conditions
In spite of the existing guidance and case law, meeting the definition of disability contained in the DDA is likely to continue to present challenges to those with autistic spectrum disorders. The Bill seeks to amend the DDA in a way which widens the scope of the existing definition in a way which would encompass autistic spectrum conditions.
In broad terms Autism has been described as follows:
Autism is a lifelong developmental disorder which affects the way people interact with the world around them. The three main areas of difficulty which all people with autism share relate to 'social communication', 'social interaction' and 'social imagination'.[15]
Autism Northern Ireland defines the disorder in the following terms:
Autism is a social and communication disability. It is not a learning disability, mental illness or health issue, although these conditions can co-exist alongside Autism.
Autism is referred to as a pervasive developmental disorder reflecting its impact across functioning levels.[16]
In clinical terms, Autism is described as:
...a neurodevelopmental disorder in the category of pervasive development disorders, and is characterised by severe and pervasive impairment in reciprocal socialisation, qualitative impairment in communication, and repetitive or unusual behaviour.[17]
Clause 4 of the Bill itself defines autism in the following way:
4.—(1) In this Act, unless the context otherwise requires—
"autism" means autism, Asperger's syndrome, Rett's syndrome, Heller's syndrome or any pervasive developmental disorder not otherwise specified;
In the UK, Ireland and other European countries, ICD-10 is the International Classification of Diseases which is most widely used and describes the internationally accepted glossary of categories of mental disorders with key sets of clinical features. The definition of autism contained within the Bill closely reflects the ICD-10 definition of Pervasive Developmental Disorders (F84).[18]
F84 Pervasive developmental disordersA group of disorders characterized by qualitative abnormalities in reciprocal social interactions and in patterns of communication, and by a restricted, stereotyped, repetitive repertoire of interests and activities. These qualitative abnormalities are a pervasive feature of the individual's functioning in all situations. |
|
F84.0 Childhood autism F84.1 Atypical autism F84.2 Rett's syndrome F84.3 Other childhood disintegrative disorder (includes Heller's syndrome) F84.4 Overactive disorder associated with mental retardation and stereotyped movements F84.5 Asperger's syndrome F84.8 Other pervasive developmental disorders F84.9 Pervasive developmental disorder, unspecified |
Definitions of each of the pervasive developmental disorders, as set out in ICD-10, are contained in Appendix 2 to this paper. It should be noted, however, that these definitions and the concept of autistic spectrum disorders itself are not unchallenged. Defining a 'social impairment' is problematic due to the difficulty in establishing diagnostic boundaries to the concept and some authors reject current classifications due to their poor evidence base and circularity.[19]
Amendment to the Disability Discrimination Act 1995
Clause 1 of the Bill amends the definition of disability contained in section 1 of the DDA. The amendment provides that the definition, which has been discussed above, will refer not only to 'physical, mental impairments' but to physical, mental or social (including communication) impairments'.
- Whilst the categorisation of impairments as either physical or mental could be considered to encompass all impairments, it could also be argued that they do not encompass impairments which are behavioural in nature, such as impairments of social functioning. In this context it is worth noting that pervasive developmental disorders are included in Chapter V of ICD-10, which covers 'Mental and behavioural disorders'. In addition to pervasive developmental disorders, the broadening of the definition has the potential to facilitate access to the protections provided by the DDA to those with behavioural disorders, such as Anxious [avoidant] personality disorder (FP60.4).
- Clause 1 of the Bill also extends the definition of 'normal day-to-day activities' in Schedule 1 of the DDA. Currently, Schedule 1 of the DDA defines 'normal day-to-day activities' in the following terms[20]:
Normal day-to-day activities
4 (1) An impairment is to be taken to affect the ability of the person concerned to carryout normal day-to-day activities only if it affects one of the following—
(a) mobility;
(b) manual dexterity;
(c) physical co-ordination;
(d) continence;
(e) ability to lift, carry or otherwise move everyday objects;
(f) speech, hearing or eyesight;
(g) memory or ability to concentrate, learn or understand; or
(h) perception of the risk of physical danger
The Bill amends this to add
taking part in normal interaction or
forming social relationships
The Equality Act 2010
The Equality Act 2010[21] which provided for the repeal of the DDA in England, Scotland and Wales, is the key piece of legislation which provides protection against discrimination on nine specific grounds. Section 6 of the Equality Act defines 'disability' in the following way[22]:
6 Disability
(1) A person (P) has disability if –
(a) P has a physical or mental impairment, and
(b) The impairment has a substantial and long-term effect on P's ability to carry out normal day to day activities.
The Equality Act definition of disability does not make reference to social impairments.
In spite of the reference to normal day to day activities in the definition above, the Equality Act, unlike the DDA, does not itself define what these are. The UK Parliament's Joint Human Rights Committee, when scrutinising the then Equality Bill, noted that these impeded access to taking cases on the grounds of disability,[23] stating:
These provisions of the Bill substantially re-enact the definition of disability contained in the DDA. However, the Bill clarifies the definition and extends protection against discrimination by removing the restrictive list of "capacities" currently set out in Schedule 1 of the DDA, which serves as an aid in defining what are "normal day-to-day activities". The Government has taken the view that this list constituted an "unnecessary extra barrier to disabled people taking cases in courts and tribunals". We welcome the deletion of the list of "capacities" from the definition of disability, which will clarify the law and make it easier for claimants to demonstrate that they are "disabled" for the purposes of the legislation.
The Office for Disability Issues, the body set up to co-ordinate disability policies across the UK Government, however, has published a consultation document on guidance for defining disability within the context of the Equality Act. The consultation opened on 9 August 2010 and closed on 31 October 2010[24]. Section D of the consultation document presented guidance on defining 'normal day-to-day activities'. The document also refers specifically to ASD in several areas:
- ASD as a developmental impairment (p.8)
- A child diagnosed with autism used as an example of a 'substantial adverse effect on his ability to carry out normal day to day activities' (p.36)[25]
- A man with Asperger's Syndrome used as an example of someone who, because of the difficulties with communication the disorder causes, is considered to be a person with an impairment that has a substantial adverse effect on normal day to day activities (p.45)[26]
An appendix to the Guidance gives a list of factors which it would be reasonable to regard as having an adverse effect on normal day to day activities, which includes the following (pp.48-9):
- Difficulty giving clear basic instructions to colleagues or providers of a service
- Difficulty asking specific questions to clarify instructions
- Taking longer than someone who does not have an impairment to say things
- Significant difficulty taking part in normal social interaction or forming social relationships
Disability Act 2005
In the Republic of Ireland, section 2 of the Disability Act 2005 uses the following definition of disability[27]:
"disability", in relation to a person, means a substantial restriction in the capacity of the person to carry on a profession, business or occupation in the State or to participate in social or cultural life in the State by reason of an enduring physical, sensory, mental health or intellectual impairment
This definition refers not only to physical and mental health impairments but also to sensory and intellectual impairments. There is no reference, however, to social or behavioural impairments. Whilst the definition in section 2 of the Disability Act 2005 refers to participation in social life, the legislation provides no further information as to what this refers.
3. Clause 2 - Autism Strategy
- Clause 2(1) of the Bill places a duty on the Department of Health, Social Services and Public Safety (DHSSPS) to prepare and publish a strategy on autism within two years of the bill becoming an Act.
- Section 1 (1) of the Autism Act is similar but the strategy is restricted to meeting the needs of adults by local authorities and the responsibility for preparation and publication of the strategy rests with the Secretary of State.
The relevant provision of the Autism (Scotland) Bill mirrors that of the Autism Act but responsibility for preparation and publication lies with the Scottish Ministers and the strategy covers all persons, not only children, and extends beyond local authorities to include NHS bodies.
Clause 2 (2) of the Bill requires the DHSSPS to consult with the Northern Ireland departments before preparing the autism strategy. The Autism Act requires the Secretary of State to consult with such persons as he or she considers appropriate. Whereas, the Autism (Scotland) Bill requires the Scottish Ministers to 'consult and seek participation of appropriate stakeholders and other persons' as they consider appropriate.
Clause 2(3) requires the DHSSPS to request that every HSC trust must provide data on the prevalence of autism in its area in order that the strategy can be published, implemented and updated. Clause 2 (4) requires the HSC trusts to provide the information requested. There are no similar legislative provisions in the other jurisdictions.
It is known that the prevalence of autism is increasing, however it is unclear whether this is due to rising awareness and improved diagnosis or a genuine increase in prevalence. It is believed that improved diagnosis, increased awareness and more specialist provision resulting from a specific diagnosis could account for some of the increase[28].
The Medical Research Council's review of autism research suggests that "there is fairly good agreement between epidemiological studies that ASD, if broadly defined, currently affects around 60 per 10,000 children under 8 and if narrowly defined, 10-30 per 10,000"[29]. A study of diagnostic trends in ASD in the South Wales Valleys has been undertaken over a 15 year period and supports a prevalence rate of 60 per 10,000 population[30].
The National Autism Plan for Children noted that in a typical local population unit of 55,000 children under 16 with 4,000 new births per year, an annual incidence of 24 new cases is implied with presentation at varying ages. This in turn suggested that there would be more than 250 children (under 16 years) with ASD at any one time in every such local health area[31].
Current estimates suggest that approximately 200 new ASD cases can be expected per year in Northern Ireland and that for every three suspected cases referred for diagnosis and assessment, one case will be confirmed. ASD "occurs more commonly in boys than girls at a ratio of 4:1, although this varies across the ASD spectrum"[32]. The DHSSPS notes however, that in addition to these cases there are an unknown number of older people still to be identified.[33]
In the absence of suitable 'benchmarking' information for Northern Ireland, the Independent Review of Autism Services, assumed that every child with either a suspected or likely diagnosis of ASD is referred from general childcare services to the proposed ASD specific specialist Trust teams and from this estimated the likely number of new cases requesting ASD specialist services per year (taking into account several factors[34]), to be as follows[35]:
- Northern Trust - 50 new cases;
- Belfast Trust - 37 new cases;
- South Eastern Trust- 37 new cases;
- Southern Trust - 44 new cases; and
- Western Trust - 35 new cases.
Clause 2(5) places a duty on the DHSSPS to review the strategy and publish a revised strategy at intervals of not more than seven years. The Autism Act requires the Secretary of State to review the autism strategy but does not contain a period within which a new strategy must be published. The same is true for the Scottish Ministers under the provisions contained with the Autism (Scotland) Bill.
The Department is required to monitor the implementation of the strategy by all the Departments (Clause 2(6)). All the Departments must co-operate with the DHSSPS as regards preparation, review and implementation of the strategy with regard to the parts that fall within their areas of responsibility (Clause 2(7), (8)). Clause 2(9) provides for the publication of an implementation report by the DHSSPS on the strategy every three years from publication.
4. Existing Strategies and Action Plans
Northern Ireland, England and Wales have either current autism strategies or action plans with a draft strategy recently published for Scotland. In the Republic of Ireland, a National Review of Autism Services is currently being undertaken by the Health Service Executive following a recognised need to review and clarify at national level the direction of health service provision for individuals with Autism. Consultation has been undertaken and a range of issues for consideration identified and it is expected that a final report will be presented to the Health Service Executive Board later in 2010 or early in 2011.
In Northern Ireland, the DHSSPS published an Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11 (June 2009). The Action Plan follows the publication of a series of documents including the Independent Review of Autism Services, the recommendations of the Bamford Review relating to ASD and its Equal Lives Report, and "other local, national and international work"[36].
The Action Plan is primarily focused towards health and social care services, however, notes the importance of partnership working to promote a person-centred approach to ASD service provision recognising that ASD is a life-long condition. [37] The Action Plan for Northern Ireland is to be taken forward by the Regional ASD Network Group under the chairmanship of Dr Stephen Bergin from the Public Health Agency, which commenced its work in April 2009. The Group is accountable to the HSC Board.[38]
With regard to the ASD Strategic Action Plan for Wales published in 2008, the approach taken has been to drive improvement across services for children, young people and adults in the areas of health, social services, and education, and expanding into the areas of housing, leisure and society in general[39]. In Wales the aim has been to take a holistic view encompassing the services offered by and across government and the voluntary sector and to include education, health, financial and social needs.[40] Wales has been heralded as the "first European nation to commit to a 'whole nation' model for delivering high-quality services and research" into ASD[41] which commenced with a new Chair in Autism Spectrum Disorders based in Cardiff University's School of Psychology.
The Strategy for Adults with Autism in England, published in March 2010, draws on the findings of the National Audit Office report Supporting people with autism through adulthood[42] and builds on the Autism Act 2009. It focuses on adults only and is designed to build on the progress already made in England in improving services for children with autism[43]. It is currently the only strategy in the UK to be linked to legislation, the Autism Act 2009, described in the Ministerial foreword as signalling "a new commitment across government to transforming the way public services support adults with autism[44]". The approach in the strategy does not depend on new investment but relies instead on ensuring mainstream services actively identify and respond to the needs of adults with autism focuses on five core areas of activity[45]:
- Increasing awareness and understanding of autism among frontline professionals;
- Developing consistent pathways for diagnosis in every area, followed by the offer of a personalised needs assessment;
- Improving access to the services and support which adults with autism need to live independently;
- Helping adults with autism into work, and
- Enabling local partners to plan and develop appropriate services for adults with autism.
- The Scottish Government recently published its draft autism strategy, Towards an Autism Strategy for Scotland (September 2010), which sets out what the Scottish Government in partnership with users, carers and professionals proposes to do to meet the needs of people with ASD. The Autism Spectrum Disorder Reference Group that led earlier work in Scotland from 2002 and 2008 and took forward recommendations in the Public Health Institute of Scotland Needs Assessment of those with ASD[46] has been reconvened and will be expanded to provide national leadership for the strategy.
5. Clause 3 – Content of the Autism Strategy
Clause 3 sets out the proposed content of the autism strategy. This section of the paper reviews Clause 3 in the context of the content of existing strategies and action plans as already referred to above.
Clause 3(1) states that the strategy 'must set out how the needs of persons with autism are to be addressed throughout their lives'. In its current ASD Strategic Action Plan, The DHSSPS recognises that:
ASD is a life long condition, and that whilst early interventions, assessment, diagnosis and support in childhood are absolutely essential, so too is coordinated planning into adulthood with the management of transition between childhood and adulthood of pivotal importance.[47]
To deliver on the life long requirements the DHSSPS notes that the Action Plan requires
The active involvement of individuals, families, carers, voluntary and community groups, together with representatives from other Northern Ireland departments to promote the development of complementary, co-ordinated services across other Departmental responsibilities including housing, education, employment,, social security and leisure activities.[48]
In a lifelong approach, the points of transition in an individual's life are recognised as important and one of the priorities of the DHSSPS Action Plan is the
...development of multi-disciplinary, multi-agency approaches to intervention and support recognising the importance of points of transition, e.g. between adolescence and adulthood, to include the need for signposting and liaison with organisations responsible for education, housing, benefit support, employment and leisure activities[49]
The strategy for Wales focuses in detail on the challenges of transitions for children and young people with ASD. It appears that it is in the area of transitions that the cross-cutting nature of services and co-operation between government departments, agencies, voluntary and community groups etc. becomes most required and most evident.
...the Welsh Assembly Government has recently convened a multi-disciplinary Transition External Reference Group to take forward the recommendations made by the Education, Lifelong Learning and Skills Committee in their review of SEN – part three of which focused wholly on transition and the Equal Opportunity Committee's review of services for disabled children and young people[50]
One of the recommendations in the current draft Scottish Strategy is to ensure that the ASD Reference Group, in collaboration with autism service providers, will identify the key determinants of service provision that result in improved quality of life for people with ASD across the spectrum and across the lifespan.[51]
Although the current DHSSPS Action Plan promotes inter-departmental co-ordination, it would seem that one of the aims of the proposed Bill is to ensure through legislation that this co-ordination across other departments happens in the manner required to deliver on the life long sevices for those with ASD. When reporting to the HSSPS Committee in 2008 on the Independent Review of Autism Services, Lord Maginnis, as Chair of the Review, noted that
" the one constraint on our inquiry was that we did not have authority – or any great welcome in some areas – when we tried to step outside the parameters that were dictated by the Department of Health, Social Services and Public Safety…there appears to be no desire for other departments to co-operate…unless that can be overcome difficulties will emerge in the future".[52]
The purpose of the Welsh Strategic Action Plan has been described as setting a clear direction of travel for the development of services in Wales by taking a person-centred approach to services and support for people with ASD and their families. It is acknowledged that this approach will only succeed with effective co-ordination at local, regional and national level[53] and has been described as a 'whole nation' model and a 'pioneering comprehensive approach' for delivering services and research into ASD.[54]
In Scotland, service redesign for people with autism commenced in 2001 with the Public Health Institute of Scotland (now NHS Health Scotland) carrying out an ASD Needs Assessment with the subsequent formation of the ASD Reference Group (referred to in the discussion of Clause 2 above) to take forward priorities for service improvement. The current draft strategy for Scotland Towards an Autism Strategy for Scotland (September 2010) notes the good work so far in Scotland and focuses on the ASD Reference Group now providing national leadership to promote good practice for local agencies working together and the advantages of sharing budgets. This direction would seem to cover all aspects of life for those with ASD and to encourage the development of services that cross health/social care, educational and skills development boundaries.
In the Republic of Ireland, the Disability Act 2005 has seen a change in the entitlements for individuals with disabilities including those with autism and there has been ongoing learning regarding best practice in terms of assessment and intervention services for people with autism. Consultation by the Health Service Executive in relation to models of service provision, gaps in services and other issues has identified a number of issues for further consideration including the mapping of existing services, identification of gaps in service, identification of assessment tools and best practice in relation to 0-18 year olds and others.
Two subgroups have been formed, one to review the issues concerning children with autism spectrum disorders and the other to review issues relating to services to adults with autism spectrum disorders.
Clause 3(2) prescribes that the autism strategy for Northern Ireland shall include the health care, educational and social needs of persons with autism. The current DHSSPS Action Plan focuses primarily on health and social care services for those with ASD and is designed around five key themes as follows[55]:
Service redesign to improve care, including such areas as improving co-ordination of assessment, diagnosis, care and support; and development of specialist teams at local level linked to a regional multi-disciplinary ASD group;
Performance improvement of autism services, including reducing waiting times for assessment, diagnosis and treatment;
Training and raising awareness to support parents and professionals;
Improving communication and information provided to individuals and families; and
Effective engagement and partnership working within Government and with voluntary/community groups and other agencies as required.
The five themes are all linked to the central tenet of the Care Pathway for ASD (at Appendix 3). Standards and measurable performance indicators will be developed for key stages along the Care Pathway.
A key element of the service redesign is the development of local specialist teams and a HSC Trust led local integrated network in each of the five Trusts to assist in assessment, diagnosis and interventions with close linkage to the ASD regional group network, mentioned previously in the discussions of Clause 2. Nominated lead Directors and co-ordinators have been identified in each HSC Trust. The local multi-disciplinary network in each Trust will link to the ASD Regional Network Group, which is responsible for the development of the care pathway, regional standards and performance indicators.[56]
The overall direction for service redesign in the Action Plan for Wales is based on the specific approach recently taken in Wales for developing all health and social services based on the concept of a four level/four tier strategic conception of their functions. It "recognises that it is neither appropriate nor feasible that all people with ASD should only be diagnosed, assessed and provided with interventions by the most specialised of services"[57]:
Tier 1 = direct access to first level services;
Tier 2 = more specialised but essentially local assessments and interventions from a variety of sectors;
Tier 3 = Access to regional specialist services for those with complicated diagnosis and assessment or challenging and variable comorbidities; and
Tier 4 = More specialist inpatient services or access to residential schooling (e.g. those with very limited verbal communication skills).
It places emphasis on multi-disciplinary and holistic person-centred assessment for those diagnosed or suspected of having ASD and their families, with the "recognition that a person may have special health, education or social needs".
The key worker is advocated in the Action Plan for Wales as "identified staff are empowered to work with families, carers and professionals of people with ASD…usually a professional who already provides some service to the family or carers and takes on the co-ordination role additional to their core profession"[58].
There are now 22 identified ASD leads in Wales who are a point of contact for families and professionals at a local level.[59]
Outside of health and social care, some of the main areas the Welsh strategy focuses on are[60]:
- Mapping prevalence, needs and services by an ASD Champion to carry out this mapping exercise through the Children and Young People's Partnerships and Local Health, Social Care and Well-being Strategy Groups as part of their wider mapping of needs and services, and needs assessments;
- The Children and Young People's Partnerships and Local Health, Social Care and Well-being Strategic Partnerships supporting the establishment of an ASD co-ordinating group in each local area (multi-agency and including service users and carers);
- The publication of Quality Standards in Education for Pupils with ASD in 2008, by the Welsh Assembly Government; and
- Commissioners and service providers to ensure there are "clear arrangements for transition between services for children and young people and adult services"[61]. This is supported by a number of additional key transition workers to provide support to children and young people with SEN (including those with ASD) as they move through school to further education or the workplace.
Within the current English strategy for adults with ASD, two of the five core areas of focus are relevant to health and social care needs - the development of a clear, consistent pathway for diagnosis in every area, which is followed by the offer of a personalised needs assessment, and improving access to the services and support needed to live independently in the community. Some of the main actions in these areas are linked to[62]:
- Increasing capacity around diagnosis as diagnosis is important for adults who have not had their condition recognised earlier in life;
- Ensuring diagnosis is recognised as a reason for a community care assessment;
- Development of a model care pathway to allow commissioners to develop referral and care pathways in their areas;
- Enabling adults with autism to benefit from personalisation of the social care, including access to direct payments; and
- Improving transition planning to give people with autism the right start in their adult life.
Of the remaining core areas two focus on the wider spectrum of needs including helping adults with autism into work by ensuring they can benefit from wider employment initiatives and engaging employers[63]; and enabling local partners to plan and develop appropriate services for adults with autism to meet identified needs and priorities, such as enabling adults with autism to have greater choice and control over where and how they live.[64] The draft strategy for Scotland focuses on outlining what still needs to be done in Scotland to build on the work already achieved by the ASD Reference Group to date and lists 26 specific recommendations for action, many of which cover the areas of health, education and social needs people with autism, for example[65]:
Recommendation 5 – The ASD reference group in collaboration with autism service providers will identify the key determinants of service provision that result in improved quality of life for people with ASD, across the spectrum and across the lifespan;
Recommendation 10 – It is recommended that an assessment of national waiting lists is undertaken to clarify the extent of delays and the ASD Reference Group considers and responds to these findings;
Recommendation 12 – It is recommended that the ASD Reference Group explore the ways diagnostic processes for adults and children are different and how this should inform practice;
Recommendation 14 – It is recommended that agencies and services develop a menu of interventions including therapeutic interventions and counselling for children, young people and adults with an ASD;
Recommendation 20 – It is recommended that the supported employment framework for Scotland is evaluated in terms of its impact on employment and employability for people with autism; and
Recommendation 26 – It is recommended that good practice transition guidance is developed, building on from existing educational guidance, in order to support the lifelong challenges facing people with autism as they make daily and life-stage transitions.
Clause 3(3) prescribes that the strategy for Northern Ireland must set out how the needs of families and carers for persons with autism are to be addressed.
Within the current DHSSPS Action Plan, the principles of family support services for individuals with ASD and their families will be informed by the strategic context set out in Families Matter: Supporting Families in Northern Ireland (March 2009).[66] The Action Plan highlights the main aspects of family support as[67]:
- Needs led with a clear focus on the wishes of the family;
- Support services should be accessible and flexible in respect of location, timing, changing needs etc.;
- A range of support services should cover early years, pre and post diagnosis, befriending, social support, citizenship/learning for life and parenting programmes; and
- Measures of success should be built into the provision of family support services.
In addition a key action is the production of a communication plan to provide information to people with ASD, their families and carers on developmental milestones, innovative ways of supporting individuals with ASD, and access to information on disability and services.[68]
The Family and Carer support services section[69] of the Welsh Strategy focuses specifically on the role that families and carers play in caring for (including a therapeutic input), advocating for and supporting people with ASD,
There is abundant evidence that families provide the mainstay of day-to-day care for their relatives who have ASD. They should receive effective and appropriate services and support that are flexible and responsive to the breadth and depth of their needs and circumstances.[70]
Within the English Strategy for adults, providing relevant information to adults with autism and their families at the point of diagnosis has been identified as a key matter, including information about autism and information about sources of help for the individual and their family, from telephone help lines to local voluntary groups. Statutory guidance is to provide the detail of the type of information required.[71]
The current draft strategy for Scotland sees individuals, families and carers as co-producers of planning and decision-making about the best use of funding for ASD services in the "tight financial climate"[72] and highlights the success to date of its Local Area Coordination and ASD Co-ordinator/Lead Officer posts . The Local Area approach promotes the rights of people with support needs to live ordinary lives within their local communities. Local Area Co-ordinators engage "with the most isolated people within our communities, in many cases people on the autism spectrum, who may not be accessing social care services". In addition there is also support for those with ASD from several ASD Co-ordinator posts.[73]
Clause 3(4) and (5) deal with the issue of awareness. Clause 3(4) prescribes that the autism strategy for Northern Ireland must set out proposals for promoting an autism awareness campaign and Clause 3(5) the steps the DHSSPS proposes to take to ensure that all Northern Ireland Civil Service staff who deal directly with the public are given autism awareness training. It is worth noting that Clause 3(5) as written does not appear to cover the public servants who deal directly with the public in relation to ASD who are not Civil Servants, for example, teachers and health and social care professionals.
- 'Training and raising awareness' is one of the five key themes of the current DHSSPS Action Plan. It is being delivered by the Regional ASD Group in collaboration with Local ASD Network and partner organisations via an ASD Training Strategy with the aim of sharing best practice and promoting early recognition of ASD and knowledge of referral pathways for GPs, health visitors, school nurses etc. The training aspect is specialist training for staff in frontline posts and options such as internet based support systems for training parents and professionals.[74]
- Within the Welsh Strategy, commissioners and service providers in health, social care and education sectors are to support the provision of ASD awareness training for all professionals who may come into contact with people with ASD. This is to include consideration of the development of a web-based self-instructional awareness training package for families and practitioners in Wales. In addition, professionals in the following services are to receive awareness training:
- Job Centres, Careers Offices and Employment Training Agencies;
- Further and Higher Education Institutions;
- The Youth and Criminal Justice System;
- Leisure Services; and
- Commissioners of Services.[75]
- One of the five core themes of the English Strategy for adults is 'increasing awareness and understanding of autism among front-line professionals' in line with the needs of their job with specialist training for staff in health and social care. The Department of Health, through statutory guidance, plans to work with partners to develop effective training modules and approaches which can be used by local authorities and primary care trusts to create training programmes locally. It is also "expected that autism awareness training is included in the equality and diversity planning and single equality schemes of all central government departments".[76]
A key development in this area in Scotland was in 2006 when the Scottish Government funded the National Autistic Society in 2006 to develop a complementary information resource, Next Steps, which was distributed through educational settings when a child is believed to have ASD. The pack aims included[77]:
- Increase understanding, knowledge and awareness of autism spectrum disorder (ASD);
- Ensure that parents, families and individuals with an ASD can access relevant information and services; and
- Improve general awareness of autism and provide advice to health, education and care professionals working in the field.
The draft strategy for Scotland also refers to the advantage of having the Lead Officer posts, referred to above, in gaining increased public awareness of autism and in developing and sustaining local supports. It recommends that the ASD Reference Group for Scotland explores the benefits of the Lead Officers to establish how rollout across Scotland might be best achieved.[78]
Clause 2 (6) provides that the Department may make regulations as regards the content of the autism strategy. Both the Autism Act 2009 and the Autism (Scotland) Bill contain provisions which require the Secretary of State and the Scottish Ministers respectively to issue guidance relating to implementation of the relevant strategies. Before publishing guidance, consultation must take place with and in each case guidance must address:
(a) the provision of relevant services for the purpose of diagnosing autistic spectrum conditions
(b) the identification of persons with such conditions;
(c ) the assessment of the needs of persons with such conditions for relevant services;
(d) planning in relation to the provision of relevant services to persons with autistic spectrum conditions as they move from being children to adults;
(e ) other planning in relation to the provision of relevant services to persons with autistic spectrum conditions;
(f) the training of staff who provide relevant services to persons with such conditions;
(g) local arrangements for leadership in relation to the provision of relevant services to persons with such conditions
It should be noted that the references to 'persons' relate to adults only under the Autism Act 2009.
6. Financial Effects of the Bill
The Explanatory and Financial Memorandum of the Autism Bill states that the bill will not have significant financial implications. The implementation of any strategy is where the main financial implications lie.
The Financial Memorandum of the Autism (Scotland) Bill places the cost of the Bill at 'no more than £5,000' for the Scottish Government to prepare, consult on, and publish an autism strategy. It does not infer the costs of implementing the Bill's provisions.[79]
The current DHSSPS Action Plan is supported by an extra £2.02 million to underpin the three year plan (208/09-2010/11). This forms part of the additional resource of £17million for learning disability services including respite care. The DHSSPS advocates that the Action Plan directs resources to front-line services and encourages the reorganisation of existing service capacity where possible.[80] In a news release on 29th November 2010, the Minister for Health, Social Services and Public Safety announced an additional £100,000 to develop specialist adult diagnostic services in addition to the extra investment of £1.54million which was made over the 2009 – 2011 period bringing the recurrent total new investment for autism services to £1.64million from April 2011.[81]
The Welsh Government has committed £5.4 million to the implementation of its Strategic Action Plan over the first three years of the 10-year plan. From 2007-08, the recurrent sum of £1.7 million has continued to be available through the revenue support grant to local authorities, specifically to develop specialist services for children with autism.[82]
The Strategy for adults with autism in England has a different approach and "does not depend on new investment", rather the aim is to identify how to make existing policies work better for adults with autism and relies on ensuring that mainstream services actively identify and respond to the needs of adults with autism. This approach "reflects the fact that there is already a wealth of government policy and initiatives that should support adults with autism".[83]
Appendix 1 Provisions of the Autism Act 2009, the Autism (Scotland) Bill and the Autism (Northern Ireland) Bill that refer to the provision of an autism strategy.
| Autism Act | Scotland | Northern Ireland | ||
|---|---|---|---|---|
| Strategy preparation and publication | Strategy to improve provision 1(1) | Strategy to improve provision 1(1) | Strategy 2(1) | |
| Timescale | By 1 April 2010 1(3) | Within 4 months 1(3) | Not less than 2 years 2(1) | |
| Review and revision | Publish if revised 1(5) | Publish if revised 1(5) | Publish revised strategy every 7 years | |
| Consultation | With such persons as considered appropriate 1(6) | Consult and seek participation of appropriate stakeholders 1(6) | Consult NI Departments 2(2) | |
| Data | Must be provided by every HSC trust 2(4) | |||
| Guidance/content | Guidance to local authorities and NHS bodies 2(1) | Guidance to local authorities and NHS bodies 2(1) | Strategy content 3(6) | |
| Monitoring | Review effectiveness 2(4) | Review effectiveness 2(4) | Department to monitor implementation 2(6); report every three years 2(9) | |
| Strategy/guidance content | Diagnosis | Relevant services for diagnosis 2(5)(a) | Relevant services for diagnosis 2(5)(a) | |
| Identification | Adults with ASD 2(5)(b) | Adults with ASD 2(5)(b) | ||
| Needs | Assessment of needs of adults with ASD 2(5)(c) | Assessment of needs of adults with ASD 2(5)(c) | ||
| Planning | Provision of services 2(5)(d-e) | Provision of services 2(5)(d-e) | ||
| Training | For staff who provide services 2(5)(f) | For staff who provide services 2(5)(f) | For staff who have contact with people with ASD 3(5) | |
| Leadership | Local arrangements for provision of services 2(5)(g) | Local arrangements for provision of services 2(5)(g) | ||
| Addressing of needs | How needs are to be addressed 3(1-2); and those of family and/or carers 3(3) | |||
| Awareness raising | Awareness campaign 3(4) | |||
Appendix 2: World Health Organisation Definition of Pervasive Developmental Disorders
F84 Pervasive Developmental Disorders
F84.0 Childhood autism
A. Presence of abnormal or impaired development before the age of three years, in at least one out of the following areas:
(1) receptive or expressive language as used in social communication;
(2) the development of selective social attachments or of reciprocal social interaction;
(3) functional or symbolic play.
B. Qualitative abnormalities in reciprocal social interaction, manifest in at least one of the following areas:
(1) failure adequately to use eye-to-eye gaze, facial expression, body posture and gesture to regulate social interaction;
(2) failure to develop (in a manner appropriate to mental age, and despite ample opportunities) peer relationships that involve a mutual sharing of interests, activities and emotions;
(3) A lack of socio-emotional reciprocity as shown by an impaired or deviant response to other people's emotions; or lack of modulation of behaviour according to social context, or a weak integration of social, emotional and communicative behaviours.
C. Qualitative abnormalities in communication, manifest in at least two of the following areas:
(1) a delay in, or total lack of development of spoken language that is not accompanied by an attempt to compensate through the use of gesture or mime as alternative modes of communication (often preceded by a lack of communicative babbling);
(2) relative failure to initiate or sustain conversational interchange (at whatever level of language skills are present) in which there is reciprocal to and from responsiveness to the communications of the other person;
(3) stereotyped and repetitive use of language or idiosyncratic use of words or phrases;
(4) abnormalities in pitch, stress, rate, rhythm and intonation of speech;
D. Restricted, repetitive, and stereotyped patterns of behaviour, interests and activities, manifest in at least two of the following areas:
(1) an encompassing preoccupation with one or more stereotyped and restricted patterns of interest that are abnormal in content or focus; or one or more interests that are abnormal in their intensity and circumscribed nature although not abnormal in their content or focus.
(2) apparently compulsive adherence to specific, non-functional, routines or rituals;
(3) stereotyped and repetitive motor mannerisms that involve either hand or finger flapping or twisting, or complex whole body movements;
(4) preoccupations with part-objects or non-functional elements of play materials (such as their odour, the feel of their surface, or the noise or vibration that they generate);
(5) distress over changes in small, non-functional, details of the environment.
E. The clinical picture is not attributable to the other varieties of pervasive developmental disorder; specific developmental disorder of receptive language (F80.2) with secondary socio-emotional problems; reactive attachment disorder (F94.1) or disinhibited attachment disorder (F94.2); mental retardation (F70-F72) with some associated emotional or behavioural disorder; schizophrenia (F20) of unusually early onset; and Rett's syndrome (F84.2).
F84.1 Atypical autism
A. Presence of abnormal or impaired development at or after age three years (criteria as for autism except for age of manifestation).
B. Qualitative abnormalities in reciprocal social interaction or in communication, or restricted, repetitive and stereotyped patterns of behaviour, interests and activities (criteria as for autism except that it is not necessary to meet the criteria in terms of number of areas of abnormality).
C. The disorder does not meet the diagnostic criteria for autism (F84.0).
Autism may be atypical in either age of onset (F84.11) or phenomenology (84.12), these two types being differentiated with a fifth character for research purposes. Syndromes that are atypical in both respects should be coded F84.12.
F84.10 Atypicality in age of onset
A. Does not meet criterion A for autism. That is, abnormal or impaired development is evident only at or after age three years.
B. Meets criteria B, C, D and E for autism (F84.0).
F84.11 Atypicality in symptomatology
A. Meets criterion A for autism (i.e. presence of abnormal or impaired development before the age of three years).
B. Qualitative abnormalities in reciprocal social interactions or in communication, or restricted, repetitive and stereotyped patterns of behaviour, interests and activities (criteria as for autism except that it is not necessary to meet the criteria in terms of number of areas of abnormality).
C. Meets criterion E for autism.
D. Does not meet the full criteria B, C and D for autism (F84.0).
F84.12 Atypicality in both age of onset and symptomatology
A. Does not meet criterion A for autism. That is abnormal or impaired development is evident only at or after the age of three years.
B. Qualitative abnormalities in reciprocal social interactions or in communication, or restricted, repetitive and stereotyped patterns of behaviour, interests and activities (criteria as for autism except that it is not necessary to meet the criteria in terms of number of areas of abnormality).
C. Meets criterion E for autism.
D. Does not meet the full criteria B, C and D for autism (F84.0).
F84.2 Rett's syndrome
A. Apparently normal prenatal and perinatal period and apparently normal psychomotor development through the first six months and normal head circumference at birth.
B. Deceleration of head growth between five months and four years and loss of acquired purposeful hand skills between six and 30 months of age that is associated with concurrent communication dysfunction and impaired social interactions and appearance of poorly coordinated/unstable gait and/or trunk movements.
C. Development of severely impaired expressive and receptive language, together with severe psychomotor retardation.
D. Stereotyped midline hand movements (such as hand wringing or washing) with an onset at or after the time that purposeful hand movements are lost.
F84.3 Other childhood disintegrative disorder
A. An apparently normal development up to the age of at least two years. The presence of normal age-appropriate skills in communication, social relationships, play, and adaptive behaviour at age two years or later is required for diagnosis.
B. A definite loss of previously acquired skills at about the time of onset of the disorder. The diagnosis requires a clinically significant loss of skills (and not just a failure to use them in certain situations) in at least two out of the following areas:
(1) expressive or receptive language;
(2) play;
(3) social skills or adaptive behaviour;
(4) bowel or bladder control;
(5) motor skills.
C. Qualitatively abnormal social functioning, manifest in at least two of the following areas:
(1) qualitative abnormalities in reciprocal social interaction (of the type defined for autism);
(2) qualitative abnormalities in communication (of the type defined for autism);
(3) restricted, repetitive and stereotyped patterns of behaviour, interests and activities including motor stereotypies and mannerisms;
(4) a general loss of interest in objects and in the environment.
D. The disorder is not attributable to the other varieties of pervasive developmental disorder; acquired aphasia with epilepsy (F80.6); elective mutism (F94.0); schizophrenia (F20-F29); Rett's syndrome (F84.2).
F84.4 Overactive disorder associated with mental retardation and stereotyped movements
A. Severe motor hyperactivity manifest by at least two of the following problems in activity and attention:
(1) continuous motor restlessness, manifest in running, jumping and other movements of the whole body.
(2) marked difficulty in remaining seated: will ordinarily remain seated for a few seconds at most except when engaged in a stereotypic activity (see criterion B).
(3) grossly excessive activity in situations expecting relative stillness.
(4) very rapid changes of activity, so that in general activities last for less than a minute on end (occasional longer periods on highly favoured activities do not exclude this; and very long periods spent in stereotypic activities can also be compatible with this problem being present at other times).
B. Repetitive and stereotyped patterns of behaviour and activity manifest by at least one of the following:
(1) fixed and frequently repeated motor mannerisms: these may involve either complex movements of the whole body or partial movements such as hand-flapping.
(2) the excessive and non-functional repetition of activities that are constant in form: this may be play with a single object (e.g. running water) or a ritual of activities (either alone or involving other people).
(3) repetitive self-injury.
C. IQ less than 50.
D. An absence of the autistic type of social impairment, i.e. the child must show at least three of the following:
(1) developmentally appropriate use of eye gaze, expression, and posture to regulate social interaction.
(2) developmentally appropriate peer relationships that include sharing of interests, activities, etc.
(3) at least sometimes approaches other people for comfort and affection.
(4) can sometimes share other people's enjoyment. Other forms of social impairment, e.g. a disinhibited approach to strangers, are compatible with the diagnosis.
E. Does not meet diagnostic criteria for autism (F84.0 and F84.1), childhood disintegrative disorder (F84.3) or hyperkinetic disorders (F90.-).
F84.5 Asperger's syndrome
A. A lack of any clinically significant general delay in spoken or receptive language or cognitive development.
Diagnosis requires that single words should have developed by two years of age or earlier and that communicative phrases be used by three years of age or earlier. Self-help skills, adaptive behaviour and curiosity about the environment during the first three years should be at a level consistent with normal intellectual development. However, motor milestones may be somewhat delayed and motor clumsiness is usual (although not a necessary diagnostic feature). Isolated special skills, often related to abnormal preoccupations, are common, but are not required for diagnosis.
B. Qualitative abnormalities in reciprocal social interaction (criteria as for autism).
C. An unusually intense circumscribed interest or restricted, repetitive, and stereotyped patterns of behaviour, interests and activities (criteria as for autism; however it would be less usual for these to include either motor mannerisms or preoccupations with part- objects or non-functional elements of play materials).
D. The disorder is not attributable to the other varieties of pervasive developmental disorder; schizotypal disorder (F21); simple schizophrenia (F20.6); reactive and disinhibited attachment disorder of childhood (F94.1 and .2); obsessional personality disorder (F60.5); obsessive-compulsive disorder (F42).
F84.8 Other pervasive developmental disorders
F84.9 Pervasive developmental disorder, unspecified
This is a residual diagnostic category that should be used for disorders which fit the general description for pervasive developmental disorders but in which a lack of adequate information, or contradictory findings, means that the criteria for any of the other F84 codes cannot be met.
Appendix 3 – Care Pathway for ASD Services in Northern Ireland[84]
Care Pathway for ASD Services
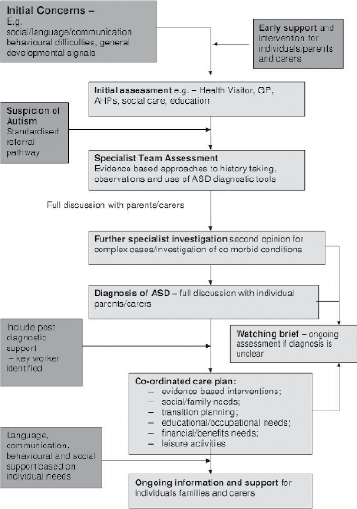
[1] Autism Bill – Explanatory and Financial Memorandum
[2] Disability Act 2005 Section 2(1).
[3] The Autistic Spectrum Disorder (ASD) Strategic Action Plan for Wales, Welsh Assembly Government, April 2008, Page 47
[4] News from Autism Cymru and Autism Speaks, www.autismspeaks.org.uk, 9th November 2007
[5] Supporting people with autism through adulthood, National Audit office, June 2009
[6] Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, Ministerial Foreward, page 4
[7] McGimpsey announces £100k funding to boost autism services DHSSPS – Press Release (29/11/10)
http://www.northernireland.gov.uk/index/media-centre/news-departments/news-dhssps/news-dhssps-291110-mcgimpsey-announces-100k.htm
[8] Autism Bill – Explanatory and Financial Memorandum
[9] Full text of the Disability Discrimination Act (the 1995 Act) can be accessed at http://www.opsi.gov.uk/acts/acts1995/Ukpga_19950050_en_1.htm#end
[10] See Autism Bill: Explanatory and Financial Memorandum.
[11] Section 1 (1) of the 1995 Act http://www.opsi.gov.uk/acts/acts1995/ukpga_19950050_en_2#pt1-l1g1
[12]http://www.ofmdfmni.gov.uk/disabilitydiscriminationact1995.pdf
[13] Hewett v Motorola 2004, UKEAT/ 0526/03: http://www.bailii.org/uk/cases/UKEAT/2004/0526_03_1602.html
[14] Graham, Autism, Discrimination and the Law (2008), p.43
[15] House of Commons Public Accounts Committee, Supporting People with Autism through Adulthood, Fiftieth Report of Session 2008-09, 15 July 2009: http://www.publications.parliament.uk/pa/cm200809/cmselect/cmpubacc/697/697.pdf.
[16]http://www.autismni.org/understanding/index.asp, accessed 6 September 2010.
[17] Susan Levy et al, 'Autism' in The Lancet (2009) 374, 1627-1638.
[18] World Health Organisation, ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic criteria for research (1993), pp.179-187.
[19] See, for example, Sami Timini et al, The Myth of Autism (2010), pp.170-1.
[20] Disability Discrimination Act 1995 Schedule 1 Paragraph 4.
[21] The Equality Act, with some minor exceptions, does not cover Northern Ireland, but a future Single Equality Act for Northern Ireland may well include much of the detail of the Westminster Act.
[22] Equality Act 2010, Section 6(1).
[23] House of Commons House of Lords Joint Committee on Human Rights, Legislative Scrutiny: Equality Bill (2009), p.49.
[24] Office for Disability Issues, Equality Act 2010: Guidance – Guidance on matters to be taken into account in determining questions relating to the definition of disability.
[25] This same example is used in the current OFMDFM guidance p.41.
[26] This same example is used in the current OFMDFM guidance p.60.
[27] Disability Act 2005 Section 2(1).
[28] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, Chapter 1, page 8
[29] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, Chapter 1, page 7
[30] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, Chapter 1, page 7
[31] National Autism Plan for Children, March 2003, National Initiative for Autism: Screening and Assessment, Executive Summary
[32]Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 7
[33]Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 7
[34] Factors included numbers living in each Trust area, birth rate patterns 2004-2007 and current ASD prevalence rates
[35] The Independent Review of Autism Services , Chaired by Lord Maginnis of Drumglass, May 2008, page 45
[36]Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 10
[37]Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 6
[38]Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 4
[39]The Autistic Spectrum Disorder (ASD) Strategic Action Plan for Wales, Welsh Assembly Government, April 2008, Page 1
[40]The Autistic Spectrum Disorder (ASD) Strategic Action Plan for Wales, Welsh Assembly Government, April 2008, Page 47
[41] News from Autism Cymru and Autism Speaks, www.autismspeaks.org.uk, 9th November 2007
[42] Supporting people with autism through adulthood, National Audit office, June 2009
[43] Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, Ministerial Foreward, page 4
[44] Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, Ministerial Foreward, page 4
[45] 'Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, page 18
[46] Public Health Institute of Scotland Autistic Spectrum Disorders Needs Assessment Report, 2001, PHIS/NHS Scotland
[47] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 6
[48] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 5
[49] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 21
[50] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, Chapter 5, page 32
[51] Towards an ASD Strategy for Scotland, The Scottish Government, 2010, page 45
[52] Committee for HSSPS, Official Report (Hansard), Independent Review of Autism Services, 3 July 2008
[53] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, Executive Summary
[54] News from Autism Cymru and Autism Speaks, www.autismspeaks.org.uk, 9 November 2007
[55] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page s 12 -17
[56] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page s 17-18
[57] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, Chapter 4, page 23-24
[58] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, Chapter 3, page 19
[59] Statement by the Welsh Assembly Government on the ASD Strategic Action Plan for Wales, Deputy Minister for Social Services, 8 June 2010
[60] Autistic Spectrum Disorder (ASD) Services, NI Assembly, Research and Library Services, Research Paper, 42/09, November 2008, pages 7-8
[61] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, Chapter 1, page 4
[62] Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, chapters 3 and 4
[63] Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, page 49
[64] Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, page 59
[65] Towards an ASD Strategy for Scotland, The Scottish Government, 2010, pages 59-62
[66]http://www.nidirect.gov.uk/families_matter_strategy.pdf
[67] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page s 11-12
[68] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page s 34-35
[69] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, pages 41-43
[70] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, paragraph 78, page 42
[71] Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, page 38
[72] Towards an ASD Strategy for Scotland, The Scottish Government, 2010, page 7
[73] Towards an ASD Strategy for Scotland, The Scottish Government, 2010, page 24
[74] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page s 32-33
[75] The ASD Strategic Action Plan for Wales (April 2008), Welsh Assembly Government, page 12
[76] Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, page 31
[77] Towards an ASD Strategy for Scotland, The Scottish Government, 2010, page 17
[78] Towards an ASD Strategy for Scotland, The Scottish Government, 2010, page 53, Recommendation 18
[79] SPICe Briefing, Autism (Scotland) Bill, 5 November 2010, page 22
[80] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 20
[81] DHSSPS News Release, McGimpsey announces £100k funding to boost autism services, 29th November 2010
[82] Statement by the Welsh Assembly Government on the ASD Strategic Action Plan for Wales, Deputy Minister for Social Services, 8 June 2010
[83] Fulfilling and rewarding lives' The Strategy for adults with autism in England (2010), Department of Health, March 2010, page 19, paragraph 1.22-1.23
[84] Autism Spectrum Disorder (ASD) Strategic Action Plan 2008/09-2010/11, DHSSPS, June 2009, page 14
17th January 2010
Autism Bill
Clause 1: Amendments to Disability Discrimination Act 1995
NIAR 000-00
Paper 000/00 17th January 2010
Research and Library Service briefings are compiled for the benefit of MLA's and their support staff. Authors are available to discuss the contents of these papers with Members and their staff but cannot advise members of the general public. We do, however, welcome written evidence that relate to our papers and these should be sent to the Research & Library Service, Northern Ireland Assembly, Room 139, Parliament Buildings, Belfast BT4 3XX or e-mailed to RLS@niassembly.gov.uk
1 Introduction
Clause 1 of the Autism Bill provides for amendments to the Disability Discrimination Act 1995 (the DDA). This briefing note, which supplements an earlier research paper on the Autism Bill, provides further information to support Members' consideration of the proposed amendments. In short, the paper:
- Addresses the relationship between the definition of disability contained within the DDA and tests of disability applied within the benefits and tax credits systems.
- Notes that in the past it has been suggested that physical and mental together are all encompassing terms and to add to them carries legislative risks.
- Highlights the relative importance of the list of day to day activities to the definition of disability and identifies support for change.
2 Relationship of definition of DDA to social security benefits and taxation
The DDA gives disabled people rights to protect them from discrimination in:
- Employment;
- Access to goods facilities and services, including transport;
- The management, buying or renting of property; and
- Education
The DDA only provides protection, however, to those people who meet its definition of disability. Disability is defined in the DDA as 'a physical or mental impairment which has a substantial and long term adverse effect on a person's ability to carry out normal day to day activities'.
It is important to note that this definition of disability is not applied within the benefits and tax credits systems. Rather, within these areas it has been noted that six main tests of disability are applied:
- limited capability for work - used for the new employment and support allowance;
- incapacity for work - used for statutory sick pay, incapacity benefit, severe disablement allowance, income support and the unemployability supplement under the Industrial Injuries and War Disablement schemes. There are different tests of incapacity depending on the benefit you claim;
- needing care, supervision or watching over by another person - used for disability living allowance care component and attendance allowance. A similar test is used for constant attendance allowance under the Industrial Injuries and War Disablement schemes;
- unable or virtually unable to walk - used for disability living allowance mobility component and war pensioners' mobility supplement;
- degree of disablement - used for industrial injuries disablement benefit, war disablement pension and vaccine damage payments;
- at a disadvantage in getting a job - used for the disability element of working tax credit. [1]
Addressing the relationship of the DDA definition to other references , guidance from OFMDFM states that:
6. The definition of disability set out in the Act and described in this guidance is the only definition relevant to determining whether someone is a disabled person for the purposes of the Act or Order. References to "disability" or to mental or physical impairments in the context of other legislation are not relevant to determining whether someone is a disabled person under the Act or Order and should be disregarded.
7. There is a range of services, concessions, schemes and financial benefits for which disabled people may qualify. These include, for example: the Blue Badge parking scheme; tax concessions for people who are blind; and disability-related social security benefits. However, each of these has its own individual eligibility criteria and qualification for any one of them does not automatically confer entitlement to protection under the Act, nor does entitlement to the protection of the Act confer eligibility for benefits or concessions.[2]
3 Physical and Mental Impairments
The DDA defines disability as 'a physical or mental impairment which has a substantial and long term adverse effect on a person's ability to carry out normal day to day activities'. Clause 1 of the Autism Bill seeks to insert 'social (including communication)' after mental into this definition.
It has been argued in the past, however, that the terms physical and mental were meant to be all encompassing and that adding further categories of impairment may not be without risk.
Addressing the suggestion that the definition should include reference to sensory impairments, William Hague, the Minister in Charge of the Disability Discrimination Bill (as the DDA was then) argued that:
... we must consider the danger of creating the impression that there ought to be additional categories, which would throw doubt on the simplicity and width of the terms "physical or mental". If the word sensory is included, people could assert that the words learning, psychiatric and psychological should be included. Those aspects are meant to be embraced by the term mental. The potential list grows even longer, but it serves only to introduce doubt about what might still be left out; the phrase "physical or mental" is meant to ensure that nothing is left out. It was wide enough in the 1944 Act, is wide enough in the Americans with Disabilities Act 1990 and, I believe, is wide enough in the Bill.[3]
Addressing the possible addition of the terms 'sensory' or 'communication' to broaden the definition of disability (as contained in the DDA) in a proposed measure of the National Assembly for Wales, The House of Commons Select Committee on Welsh Affairs noted that:
Both this committee and the Assembly Committee examined whether the term "physical or mental impairment" needed to be qualified in order to ensure that persons with a sensory or communications impairment, for example, would be included within its scope...
...The Assembly Parliamentary Service Legal Division confirmed that:
it seems clear that a communication impairment will inevitably fall under either a 'mental' or 'physical' impairment.
...Advice prepared by the Assembly Parliamentary Service Legal Division for the Assembly Committee noted:
if a definition is a broad one (as 'physical or mental impairment' appears to be) then there are risks in grafting on to it references to specific conditions which are already covered. For example, adding a specific reference to 'communication impairment' could give the impression that 'physical or mental impairment' is not as all-encompassing a definition as it would otherwise appear to be.
It is a principle of statutory interpretation that if there are a number of similar specific situations and only some of them are mentioned then the intention must be to exclude the ones which are not.[4]
4 Day to Day Activities
To meet the DDA definition of disability, an impairment must, amongst other things, affect at least one of the following 'day to day activities', which are listed in Schedule 1 of the DDA:
- mobility;
- manual dexterity;
- physical coordination;
- continence;
- ability to lift, carry or otherwise move everyday objects;
- speech, hearing or eyesight;
- memory or ability to concentrate, learn or understand; or
- perception of risk of physical danger.
The Autism Bill seeks to add 'taking part in normal social interaction' and 'forming social relationships' separately to this list. The list has in the past presented a hurdle for those with Asperger's who seek to meet the definition of disability contained in the DDA.
In the landmark case of Hewett vs. Motorola,[5] the main question addressed by the Employment Appeals Tribunal was whether the long term impairment suffered by Mr Hewett of Autistic Spectrum Disorder and/or Asperger's Syndrome affected substantially his ability to carry out normal day to day activities, and in particular his ability to concentrate, learn or understand. Remitting the case back to the Tribunal, the EAT concluded that it was in error in not accepting that the Mr Hewett's ability to understand was affected by his impairment.
Amendments to the list of day to day activities have been supported in the past. The Joint Committee on the Draft Disability Discrimination Bill published Volume 1 of their Bill Report in May 2004. Addressing the issue of day-to-day activities, the Committee concluded that:
86. A great deal of evidence suggests that the definition of "day-to-day activities" is not operating in the way in which it was originally intended. Proposed amendments by witnesses concentrated on four elements thought to be inadequately covered by the existing list: ability to care for oneself, communication, interaction with others, and perception of reality and judgement.
88. The Committee recommends the addition of the following activities to the list of "normal day-to-day activities" in Schedule 1:
- ability to care for oneself
- ability to communicate and interact with others
- perception of reality.[6]
In determining whether someone has a disability as defined in the DDA, four questions must be addressed:
(i) Has the individual got an impairment, physical or mental
(ii) Does the impairment adversely affect day to day activities?
(iii) Is the adverse effect substantial - or would it be but for the beneficial effects of ongoing medication or other treatment?
(iv) Are the adverse effects long-term?
As regards the first question above, it is important to note that it is not necessary to establish whether an impairment is physical or mental just that it is one or the other or perhaps both. Statutory guidance from the Office of the First Minister and Deputy First Minister on the definition of a disability, produced in 2008, states that:
It may not be possible, nor is it necessary, to categorise a condition as either physical or a mental impairment. The underlying cause of the impairment may be hard to establish. There may be adverse effects which are both physical and mental in nature. Furthermore, effects of a mainly physical nature may stem from an underlying mental impairment, and vice versa.[7]
It is also important to note that the first question does not take precedence over the other three. Indeed, in the context of depression and disability, it has been noted that if a tribunal finds evidence of an adverse effect it:
... should not get too hung up on labelling the particular impairment concerned... in many or most cases it will be easier –and is entirely legitimate – for the tribunal to park that issue and to ask first whether the claimant's ability to carry out normal day to day activities has been adversely effected – one might say impaired on a long term basis. If it finds that it has been, it will in many or most cases follow as a matter of common-sense inference that the claimant is suffering from a condition which has produced that adverse effect – in other words, an 'impairment'. If that inference can be drawn, it will be unnecessary for the tribunal to try to resolve difficult medical issues for the kind to which we have referred.[8]
Whilst the definition of disability in the Equality Act 2010 (the Act repealed the DDA in England Scotland and Wales) contains reference to normal day-to-day activities, the Act itself, unlike the DDA, does not stipulate what these are. The Office for Disability Issues, the body set up to co-ordinate disability policies across the UK Government, however, has published a consultation document on guidance for defining disability within the context of the Equality Act. Section D of the consultation document presented guidance on defining normal day-to-day activities and included the following within a list of factors which it would be reasonable to regard as having an adverse effect on normal day to day activities:
Significant difficulty taking part in normal social interaction or forming social relationships.[9]
17th January 2010
[1] Disability Alliance website (accessed 17/01/11) http://www.disabilityalliance.org/ask4.htm#Q13
[2] OFMDFM - Guidance on matters to be taken into account in determining questions relating to the definition of disability http://www.ofmdfmni.gov.uk/disabilitydiscriminationact1995.pdf (accessed 17/011/11)
[3] House of Commons, Disability Discrimination Bill, Standing Committee E, 2 February 1995
[4] House of Commons, Select Committee on Welsh Affairs, Second Report: Proposed Legislative Competence Orders in Council: Additional Learning Needs, 21 December 2007 available at; http://www.publications.parliament.uk/pa/cm200708/cmselect/cmwelaf/44/4402.htm
[5] Hewett v Motorola Ltd Appeal No.UKEAT/0526/03/ILB
[6] House of Commons - House of Lords, Joint Committee on the Draft Disability Discrimination Bill, Draft Disability Discrimination Bill Report, Volume 1, May 2004, available at; http://www.publications.parliament.uk/pa/jt200304/jtselect/jtdisab/82/8205.htm#a13
[7] OFMDFM, Disability Discrimination Act 1995 (as modified by Schedule 8 thereof for application in Northern Ireland) Guidance on matters to be taken into account in determining questions relating to the definition of disability, 2008, available at; http://www.ofmdfmni.gov.uk/disabilitydiscriminationact1995.pdf
[8] Michael Rubenstein, Disability: Guidance on depression cases, In the Courts: Equal Opportunities Review, December 2010
[9] Office for Disability Issues, Equality Act 2010: Guidance – Guidance on matters to be taken into account in determining questions relating to the definition of disability. p49
Paper presented by Dominic Bradley to Committee on 20.01.2011
Context2002 Task Group on Autism Report 2002 Autism Ambassadors (MLAs) 2002/04 Middletown Centre of Excellence for Autism 2004/06 The Bamford Review/ 3 HSSB Strategies on ASD/4 Board Paper 2006 The Autism Legislative Lobby 2006 The Celtic Nations Autism Partnership (CNAP) 2007 Delegations to Washington DC (NI Assembly + CNAP) 2007 DHSSPS Review of ASD Services 2008 All Party Assembly Group on Autism 2008 Health Committee delegation to Welsh Assembly 2008 Health Committee visit to ASD services for adults in N.I. 2009 Health Committee presentations by DHSSPS and APGA 2010 DHSSPS Action Plan budget cut/ DENI Action Plan for ASD consults 2010/11 Autism Bill (NI) introduced to N I Assembly |
StatisticsPrevalence rates are currently moving from 1:100 (2007) to 1:64 (Cambridge Research Centre) to 1:50 (DENI,2010)? N. Ireland: 20,000 individuals in N.I. with ASD (1:100) G. Baird Study 2006 31,000 individuals in N.I. with ASD (1:64) G. Baird Study 2009 N. Ireland: 2002 900 school children with ASD (DENI) 2007 3,500 school children with ASD (DENI) 20105,000 +?
|
Government Funding e.g. Educ v Health investment2002 Dept of Education already had ASD (WTE) specialist posts in each of 5 ELBs. 2002 – 2009 Dept of Education funds ASD Teams in 5 ELBs + Middletown + special ASD units in mainstream schools. 2002/3 DHSSPS £0.5m to Diagnostic Services 2010 DHSSPS £0.25m to implement the Autism Action |
Conclusion = poor investment
|
Recurrent Issue: Inequality
|
Recurrent Solution: Strategy with Legislation
|
Recurrent Obstacles: Cost & Bother"We can't afford legislation." "We don't need legislation, we have a strategy." "We have enough strategies and policies now." "The wider disability community will be jealous and will cry "inequality"." Each time a response has been produced....... "Legislation is affordable if it is about addressing current misspends, about reshaping and creating an ASD managed infrastructure (better housekeeping) and about creating independence and reducing dependence (better outcomes)." "Legislation and strategy are not mutually exclusive. They should be mutually dependent and supportive." "Legislation is effective if it is about building upon and making sense of existing piecemeal strategies and policies, if it is about creating a coordinated strategy that is regional and cross departmental." "Legislation will have widespread support if it is about equality for Autism. Legislation is about making our invisible citizens visible." In the end....surely it costs less to do the right thing. |
N.I Assembly Research & Library ServiceReport 1 "IMPROVING SERVICES FOR PEOPLE WITH ASD" (SEPT 2008)
N.B. The Report supports a legislation and strategy response. Report 2 "Autism Spectrum Disorders (ASD) Services" (Nov 2008)
Report 3 "The Autism Bill" (Dec 2010)
|
Evidence of Need?
- "The Hidden Community"
- "Is Anyone Listening?"
Some of the crossover issues from these investigations with families in Northern Ireland are...
- Lack of recognition (in terms of the challenges and the disability)
- Isolation
- Requirement for combative style to secure recognition and services
What is unique about ASD?
- The evidence definitely shows that the stress levels for primary carers of family members with Autism are unique within the disability community and the latest local research gives us a sliding scale from 80% to 50% of mothers who are experiencing high levels of anxiety through to those on long term medication linked to trauma and stress.
- ASD is not recognized in DDA.
- The DHSSPS Programmes of Care are inadequate. ASD is placed in Mental Health/Learning Disability POC with its budget taken from LD. This perpetuates using IQ as a gateway to services for people with ASD and therefore 75% falling outside services entitlement.
Statistics?
Add this to the rising prevalence rates which reflect a school population of around 5000 children with ASD and approx 20% of our population whose lives are directly impacted by living with Autism, then the need for a planned future and joined up resourcing to meet need is obvious.
The case I put before you today is that the historic failure to prioritise Autism appropriately is contributed to by the failure within existing legislation to recognise the disability. This anomaly is addressed within the proposed Bill.
The Autism (NI) Bill
|
Letter from Dominic Bradley
Letter from Dominic Bradley
Letter from DHSSPS 27.01.2011
Department of Education 1.02.2011
Appendix 5
List of Witnesses
Mr Dominic Bradley MLA
Arlene Cassidy Secretariat to All Party Group on Autism / Chief Executive Autism NI
Dr Maura Briscoe Mental Health & Disability Policy Directorate, DHSSPS
Dr Ian McMaster Medical Officer, DHSSPS
Dr Hilary Harrison Social Services Officer, DHSSPS
Mr Peter Deazley Learning Disability Unit, DHSSPS
Mr Charles Bamford Social Services Officer, DHSSPS
Dr Ian McMaster Medical Officer, DHSSPS
Ms Paula Hanratty Director of Family Support, Autism NI
Ms Audrey Mullan Autism Resource Officer, Autism NI
Mr David Heatley Chairperson, Parents Autism Lobby
Mr Alan Hanna Assistant Director, Autism Initiatives
Ms Grainne Close Assistant Director, Autism Initiatives
Ms Regina Cox Co-Director National Autistic Society NI
Ms Shirelle Stewart Co-Director National Autistic Society NI
Dr Tony Byrne Chairperson, Parents' Education as Autism Therapists (PEAT)
Ms Karen Gallagher Parents' Education as Autism Therapists (PEAT)
Ms Dorothy Angus Director of Access, Inclusion and Well-Being, Department of Education
Ms Debbie Gladwell, Head of Special Education Policy Advisory Team, Department of Education
Ms Gillian Boyd Department of Education Official
The Lord Maginnis of Drumglass Chairperson, RASDN Reference Group
Ms Laura Collins Member of the Regional Autistic Spectrum Disorder Reference Group
Ms Nuala White Member of the Regional Autistic Spectrum Disorder Reference Group
Appendix 6
List of Abbreviations
- DDA Disability Discrimination Act
- DHSSPS Department of Health, Social Services and Public Safety
- ASD Autism Spectrum Disorder
- RASDN Regional Autistic Spectrum Disorder Network
- SEN Special Educational Needs
- DLA Disability Living Allowance
- HSC Health and Social Board
- PAL Parent's Autism Lobby
- BELB Belfast Education and Library Board
- NEELB North Eastern Education and Library Board



